By Christian Waldherr, MD and Martin Sonnenschein, MD
Data courtesy of the Klinik Engeried, Lindenhofgruppe, Bern, Switzerland
History
A 56-year-old female who underwent total knee arthroplasty in the left knee 2 years ago presented with recent onset of pain and instability. Considering the clinical possibility of loosening, infection or overload due to incorrect positioning of the knee prosthesis, the patient was referred for a 3-phase bone scintigraphy, followed by SPECT/CT of the knee, which was performed on a Symbia Intevo™ scanner.
Initial planar dynamic and blood pool images were acquired immediately following an IV injection of 600 MBq (16.22 mCi) 99mTc MDP. Planar whole-body and SPECT/CT acquisition of the thigh were performed 3 hours post-injection. Following a thin-slice diagnostic CT (110 kV, 120 mAs CareDose™), SPECT was acquired with 60 stops per detector at 15 sec/stop. Image reconstruction using xSPECT Bone™ technology was performed using CT-based zone information. xSPECT Bone data was fused with the CT for a final evaluation.


Findings
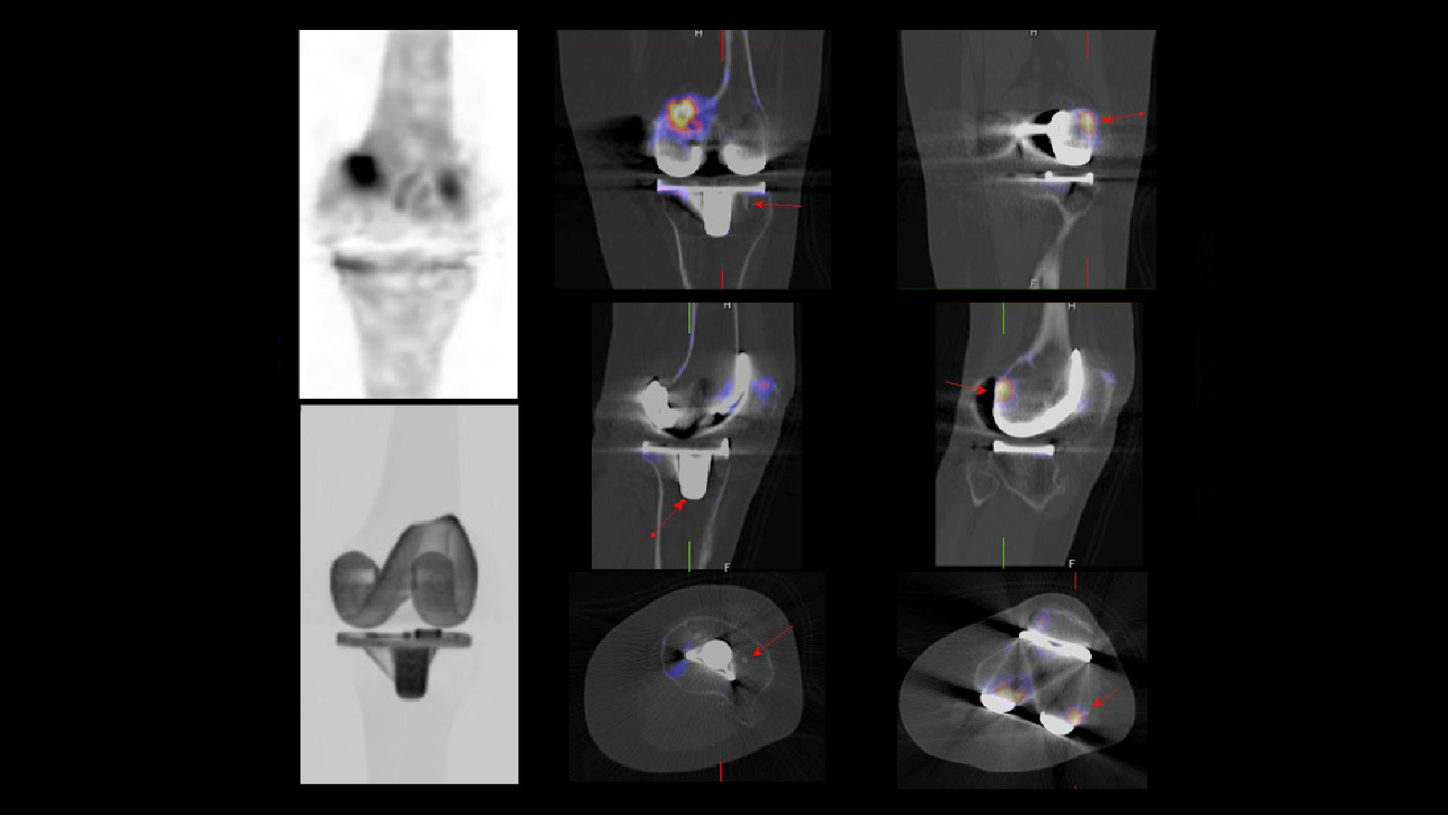
As shown in Figures 2 and 3, xSPECT Bone demonstrates focal increase in uptake within the calcified insertion of the medial head of gastrocnemius suggesting tenoperiostitis secondary to shear stress following total knee arthroplasty, which appears to be the primary cause of the left knee pain. Fused images demonstrate that the calcified inflamed tendon insertion is located just superior to the free posterior edge of the medial part of the femoral component of the knee prosthesis (Figure 2 arrow). This suggests repeated friction of the prosthesis edge with the gastrocnemius tendon insertion may have caused inflammation, thus leading to calcified tenoperiostitis. The insertion of the popliteus muscle to the lateral condyle in close proximity and just lateral to the edge of the lateral segment of femoral component of the knee prosthesis also shows focal increase in uptake, which is suggestive of tendinitis, possibly secondary to shear stress and friction with pros-thesis margins.
CT shows no gap between bone and prosthesis margins and xSPECT Bone does not show any focal abnormal uptake in the prosthesis margins except for the inflamed tendon insertions. Bone around the prosthesis stems (Figure 3 arrows) show absence of osteolysis or hypermetabolism. This indicates absence of any loosening of the prosthetic joint components, as well as absence of prosthetic infection. Maximum intensity projection (MIP) image of the CT shows proper position and alignment of the femoral and tibial component of the knee prosthesis, indicating correct position of the prosthesis and absence of stress overload due to malalignment.


Comments
Tendinitis at the insertions of muscle tendons predominantly used in joint movement is common following joint replacement surgery. This may be caused by malalignment of the prosthesis or secondary to impingement or friction with prosthetic components or loose bodies. Bone SPECT/CT successfully localizes and characterizes such enthesopathies due to the focal hypermetabolism typically associated with tendinitis. SPECT/CT also distinguishes enthesopathy from other pathologies, such as prosthetic joint loosening or stress reaction due to instability, because of the accurate localization of the site of hyper-metabolism and delineation of morphological findings like calcification in the tendon, gap between bone and prosthesis seen in loosening, or osteolysis. In this clinical example, xSPECT Bone sharply defines the focal hypermetabolism in the gastrocnemius and popliteus tendon insertions and defines the con-tours and edges of normal bone and the bone-prosthesis interface.

Conclusion
Sharp definition of skeletal hypermetabolism at tendon insertions visualized with xSPECT Bone technology, along with CT confirmation of absence of loosening, supported the diagnosis of tendinitis at gastrocnemius insertion associated with total knee arthroplasty.