History
A 72-year-old man with a history of non-Hodgkin’s lymphoma treated with chemotherapy underwent 99mTc MDP bone scan to evaluate osseous lesions. A recently performed MRI of the pelvis showed slight hyperintensity in the right femoral neck in the fat-suppressed images which was suspicious of marrow infiltration.
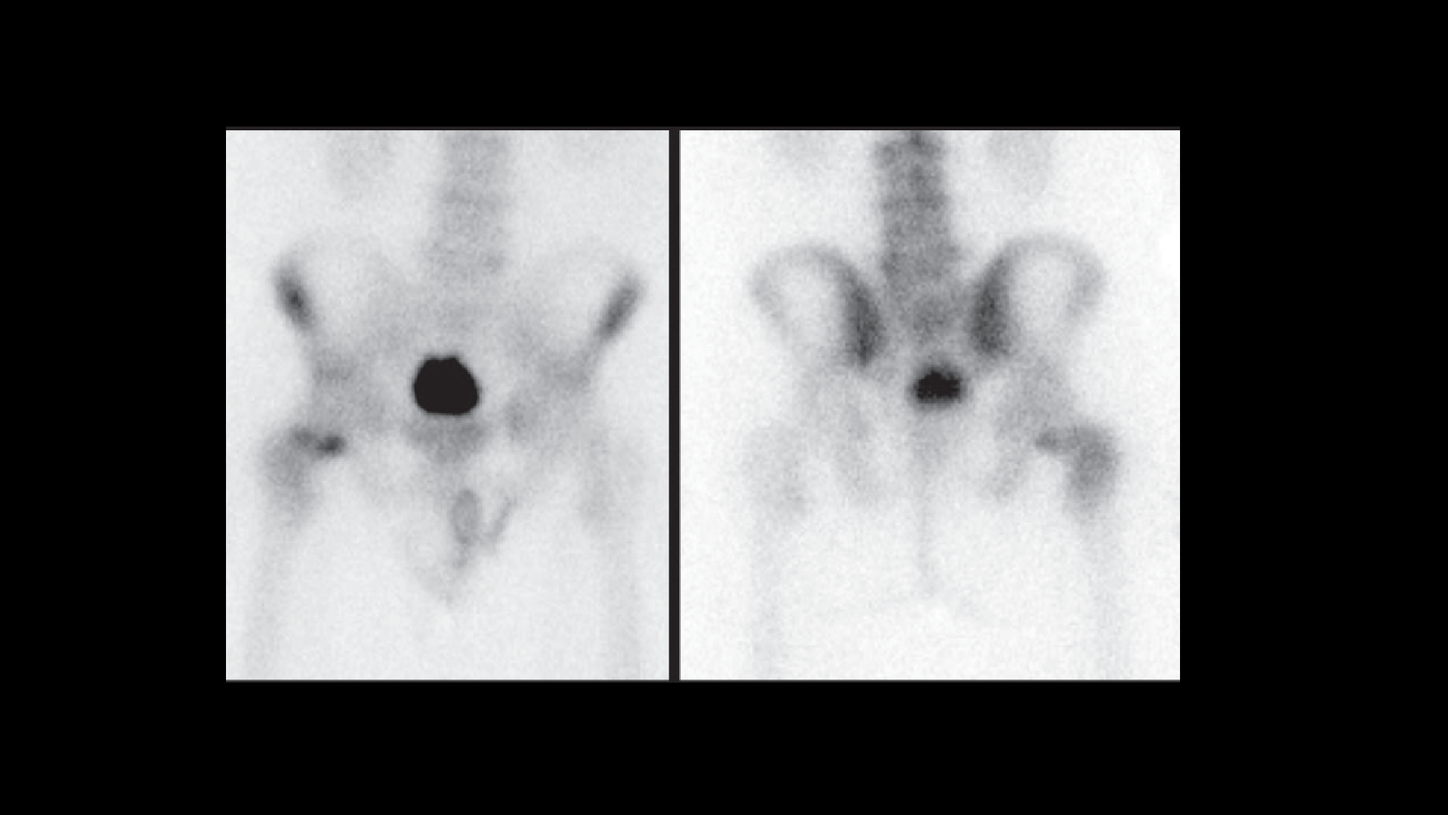
An xSPECTTM study was performed three hours following IV injection of 27.4 mCi 99mTc MDP. Initial planar images were followed by xSPECT acquisition. 3D iterative reconstruction and xSPECT BoneTM reconstructions were performed for comparison.
Findings
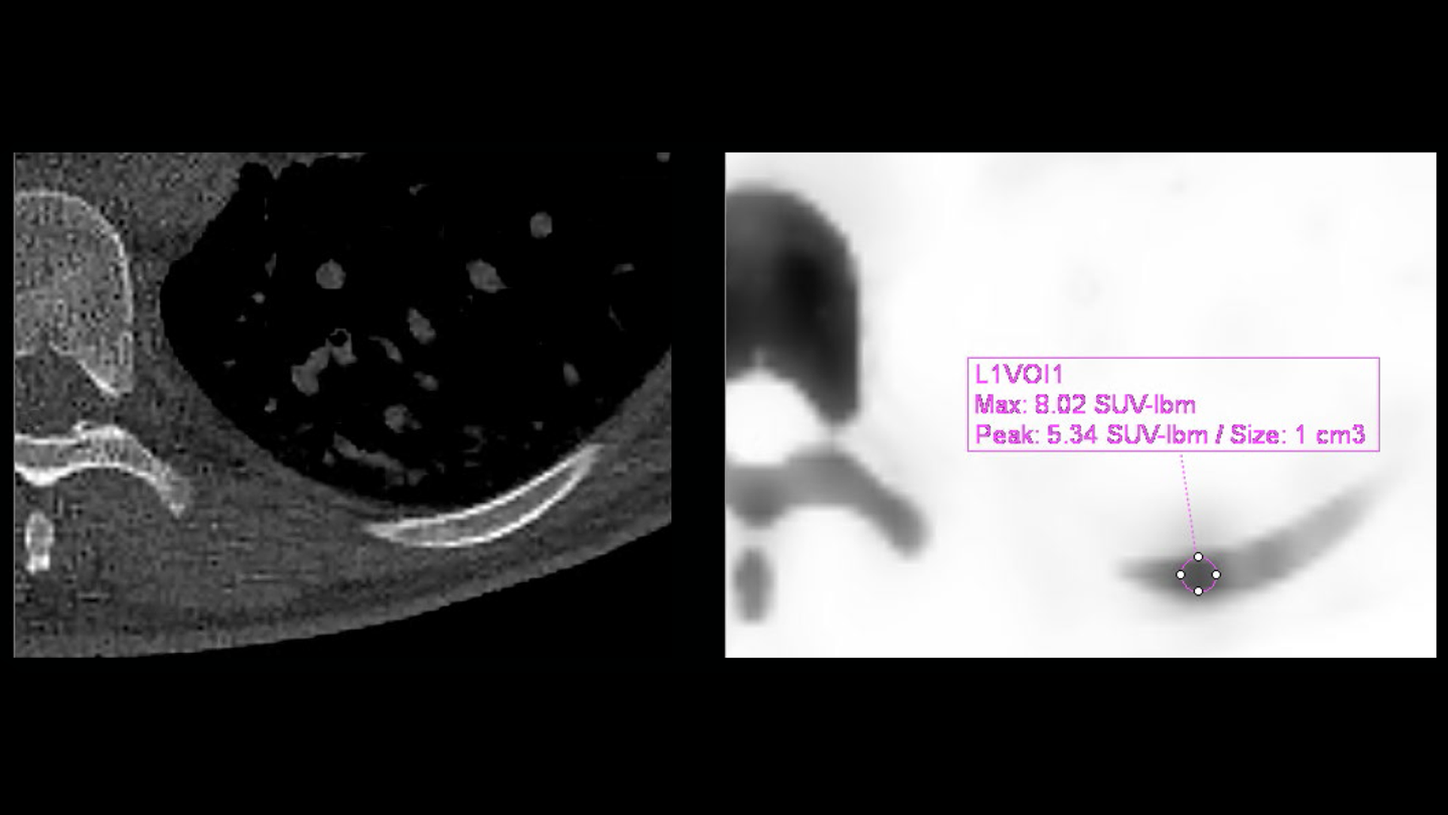
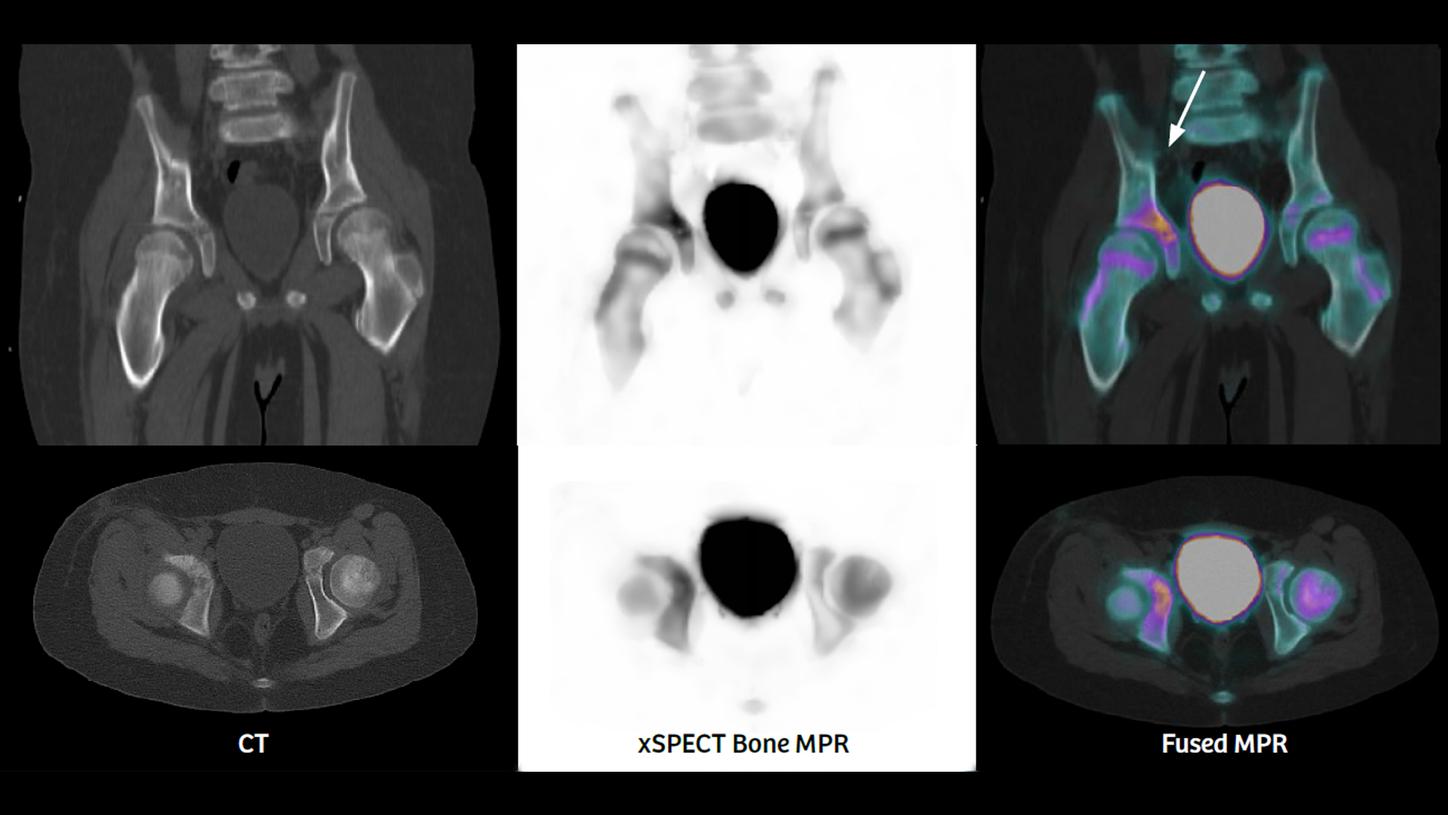
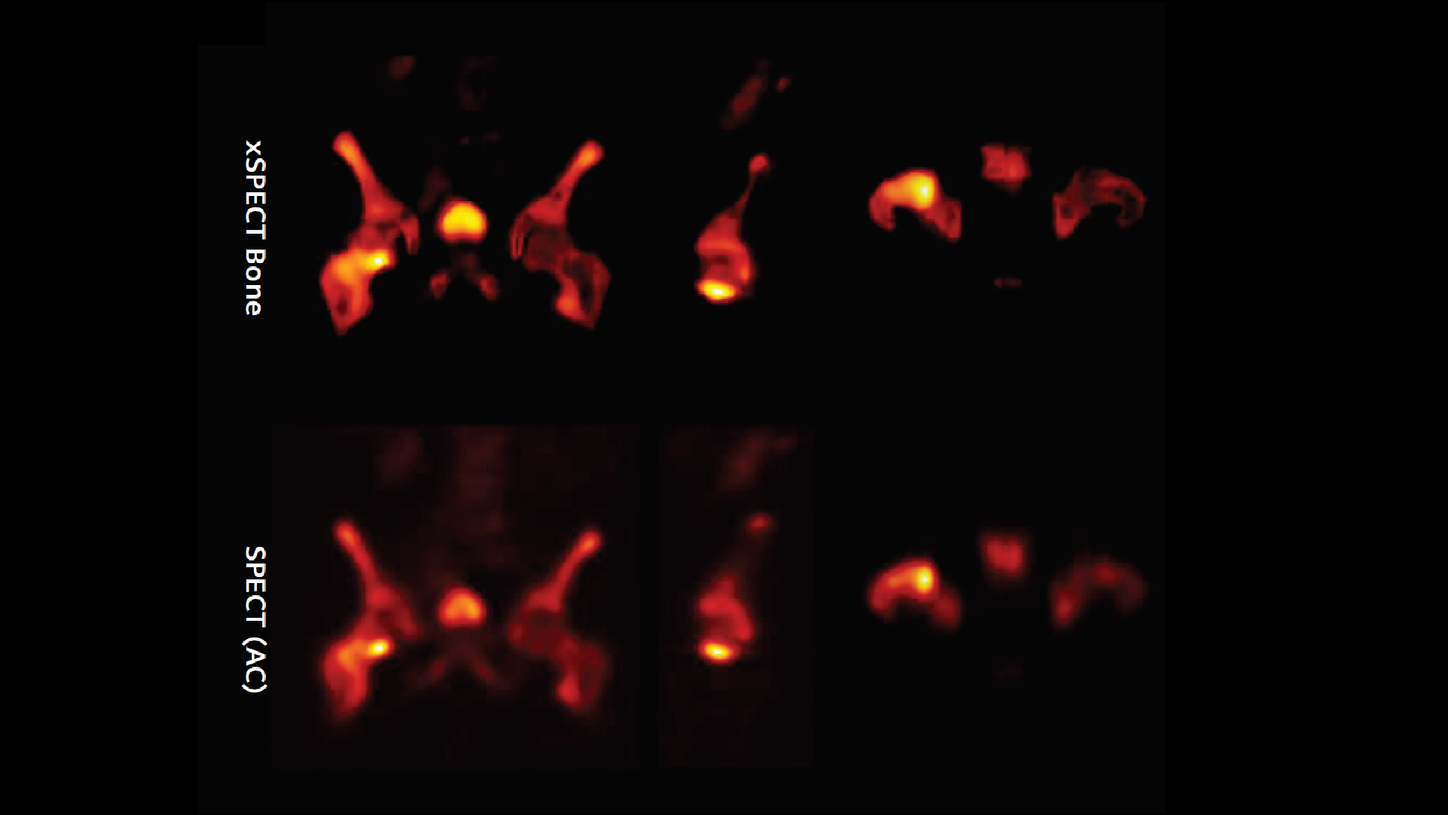
xSPECT Bone sharply defines the focal area of increased uptake in the medial margin of the neck of the femur adjacent to the femoral head. The rest of the femoral neck and the intertrochanteric crest also show slightly increased uptake. The femoral head uptake appears normal. Compared to SPECT (AC), the xSPECT Bone images show sharper margins of the hypermetabolic foci in the femoral neck as well as sharper delineation of the femoral head, trochanteric regions, intertrochanteric crest, and the rest of the pelvis and acetabulum.
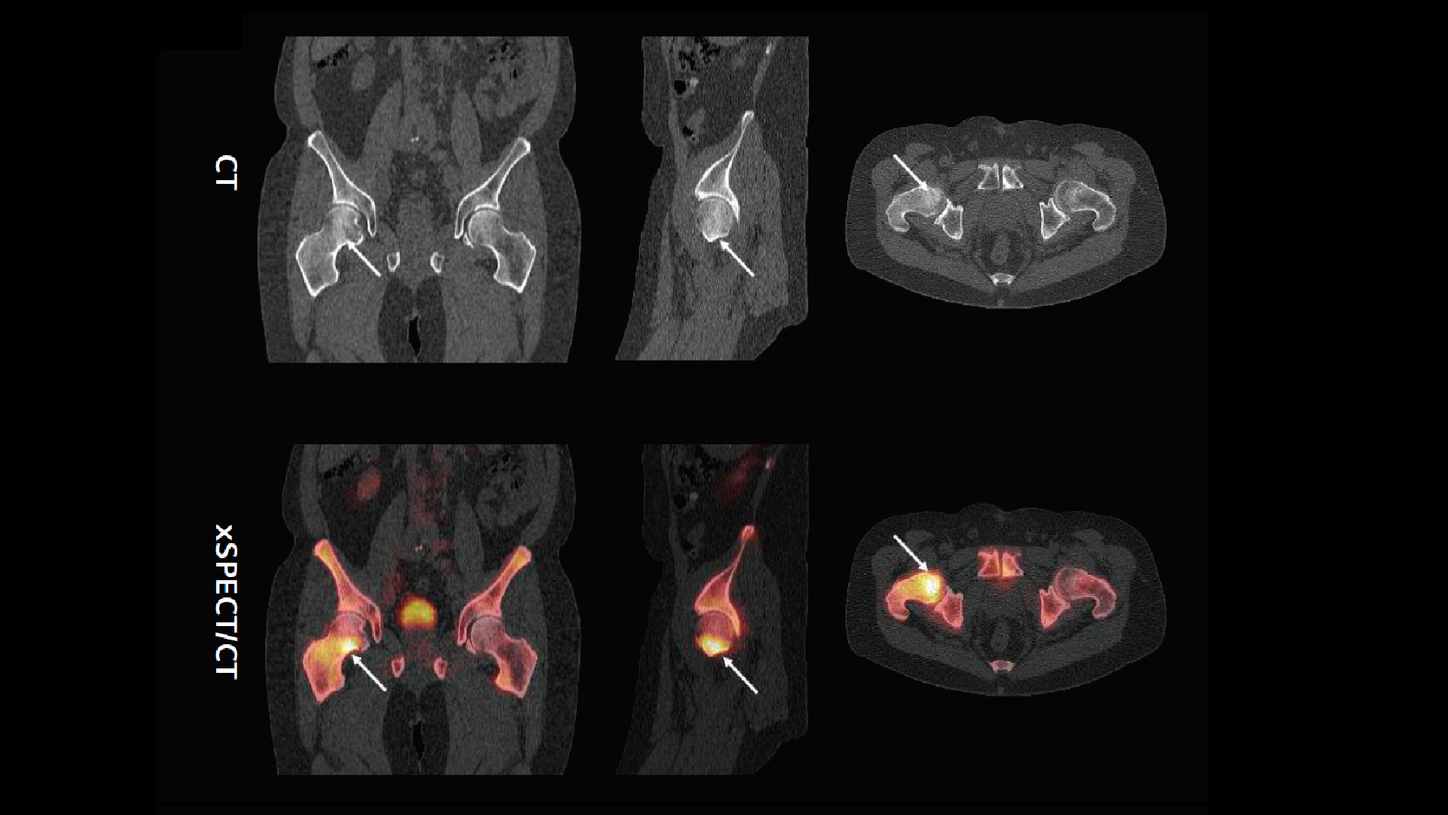
CT shows mild sclerosis involving the femoral neck just adjacent to the femoral head, predominantly in the anterior and inferior aspect of the neck. Fusion of CT with xSPECT Bone shows exact coregistration of the focal increase in uptake with the zone of sclerosis. The correlation of the focal area of skeletal hypermetabolism, along with the associated sclerosis seen on CT in view of the MRI findings at the same area, strongly suggest the presence of lymphomatous infiltration in the marrow of the femoral neck.

Comments
Marrow infiltration is common in advanced lymphoma. 18F FDG PET/CT and MRI are both highly sensitive for detection of marrow infiltration.1 In this clinical example, the MRI findings were suspicious of marrow involvement but the xSPECT Bone and CT information was supportive of the final diagnosis of lymphomatous infiltration of the femoral neck marrow. The increased sclerosis seen on CT along with the skeletal hypermetabolism may be related to osteoblastic activity stimulated by the infiltrating lymphoma cells.
Conclusion
xSPECT Bone sharply defines the extent of marrow infiltration in the femoral neck by lymphoma and correlates it with the degree and extent of sclerosis seen on CT. The well-defined boundaries of the skeletal hypermetabolism defined by xSPECT Bone provides information about the degree of involvement of the marrow of the greater trochanter and upper part of the femoral shaft beyond the heavily infiltrated region in the lower part of the femoral neck, thereby illustrating the greater extent of lymphomatous infiltration than was estimated from the CT or SPECT only.