By Michael Hoffman, MD, Associate Professor
Data courtesy of Peter MacCallum Cancer Center, Melbourne, Australia


History
An 82-year-old man with castration-resistant prostate cancer and multiple skeletal metastases demonstrated by 68Ga PSMA PET/CT to be PSMA-avid was referred for 177Lu PSMA[a] therapy. The patient was treated with an intravenous infusion of 8.7 GBq of 177Lu PSMA preceded by amino acid infusion. Five hours following therapeutic administration, the patient underwent a quantitative multibed SPECT/CT to image the distribution of 177Lu PSMA within the body. The study was performed on a Symbia Intevo™ 16. Following an initial low-dose CT acquisition (130 kV, 25 eff mAs), a three-bed SPECT/CT study using xSPECT Quant™ was acquired with 60 stops per detector and 10 seconds per stop. The study was reconstructed using xSPECT Quant to quantify 177Lu tracer concentration within the lesions and critical organs. Following the initial SPECT/CT acquisition at 5 hours post-therapy, sequential studies using identical acquisition and reconstruction protocols were performed at 24 hours and again at 96 hours.


Findings
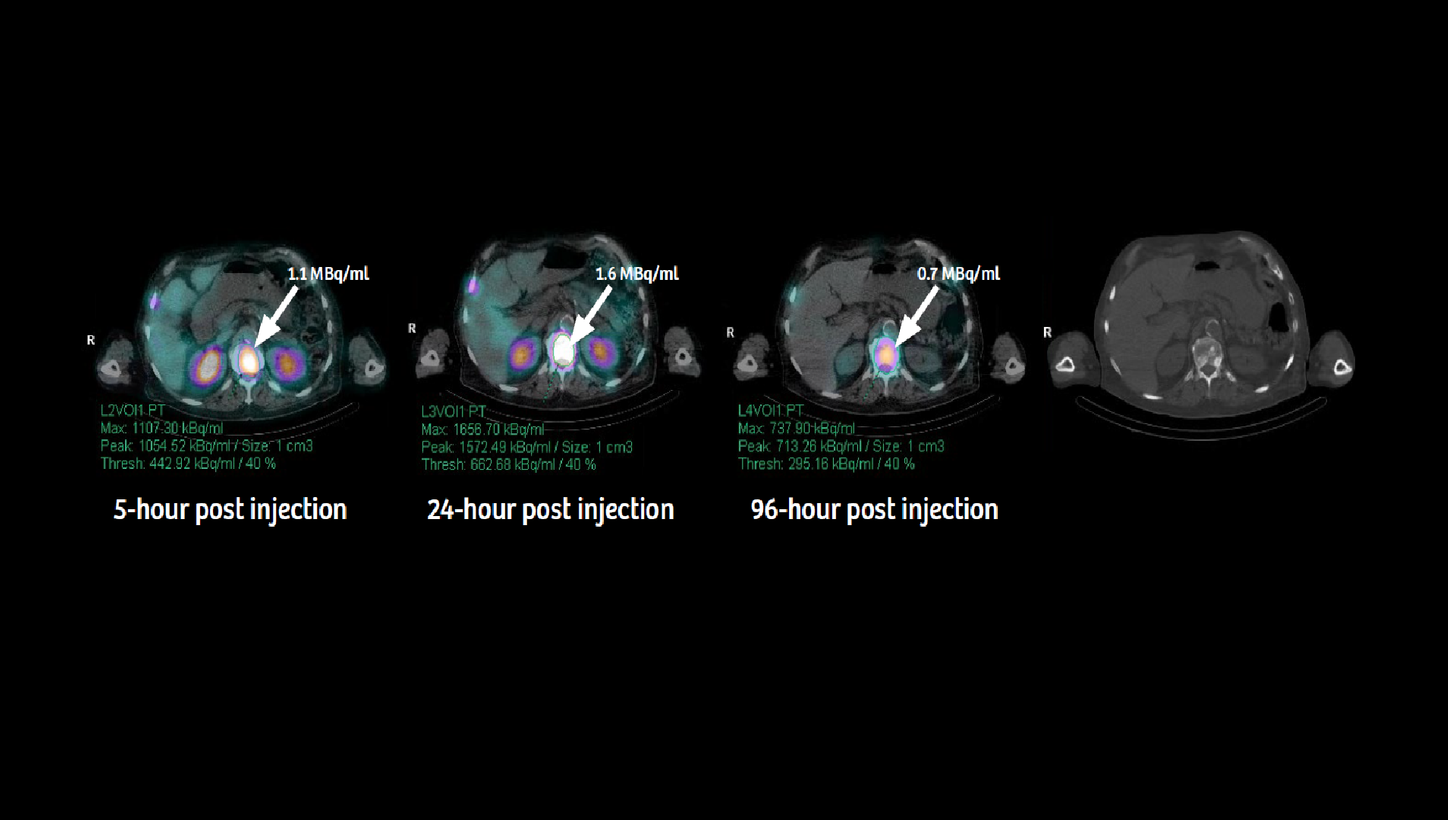
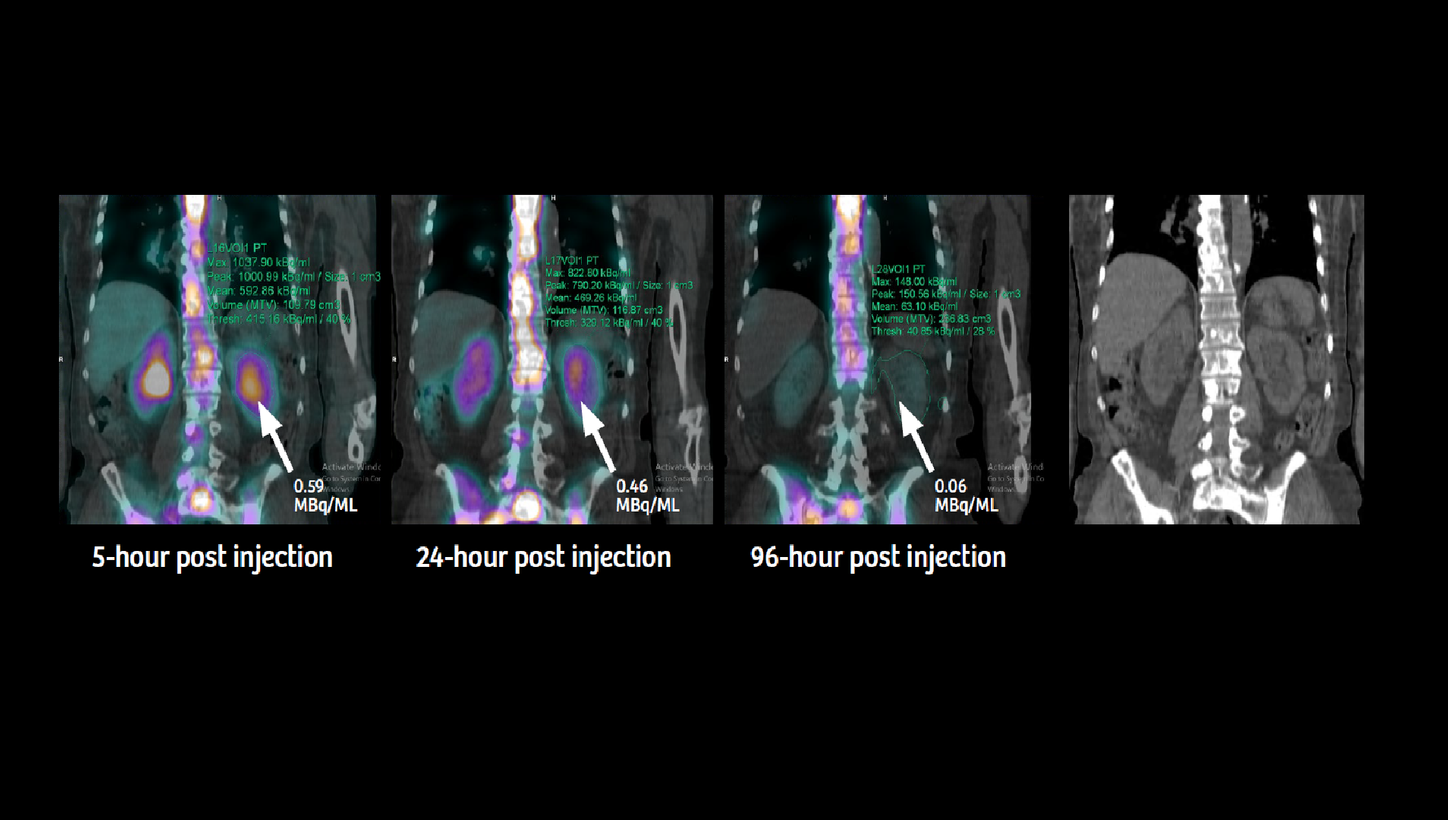
Sequential SPECT/CT images with tracer concentration values in thoracic and lumbar vertebral metastases obtained using xSPECT Quant (as displayed in Figures 1-3) clearly highlight the high initial tracer concentration within the metastases with a gradual increase in concentration up to 24 hours post injection. There was slow washout from the metastases with nearly 50% of tracer retention even at 96 hours post injection. This pattern of initial high uptake and subsequent slow washout within the metastases reflects the potential of high radiation dose delivered by 177Lu PSMA therapy.
The renal uptake appears normal in the initial 5-hour image (Figure 4) with fast washout that left only 10% of the initial concentration at 96 hours. This fast clearance suggests a low residence time of tracer within the renal cortex and a consequently low level of radiation dose to the kidneys. The normal cortical thickness and absence of pelvicalyceal enlargement on CT reflect normal renal morphology and absence of pelvicalyceal stasis or obstruction.

The sequential xSPECT Quant and CT data was fed into Siemens Healthineers’ Dosimetry Research Tool (DRT), which enables the automated generation of a volume-of-interest (VOI) that includes the tumor as well as critical organs—such as the kidney, liver, and spleen—SPECT/CT. DRT performs voxel-based dosimetry using absolute tracer concentration values obtained from sequential xSPECT Quant datasets across multiple time points. These time points calculate time-activity curves and tracer residence times within individual voxels as well as within automatically generated VOIs to generate absorbed dose values, dose volume histograms, and absorbed dose maps.
The mean left and right kidney dose (as calculated by the DRT) appears within expected levels. Due to high tracer retention within metastases and the substantial metastatic burden, the circulating tracer available for renal clearance is low and that indicates the potential for low renal cortical dose, also known as a tumor sink effect. This is appropriately reflected in the mean renal dose of 2.52 Gy and 3.6 Gy to the left and right kidneys, respectively. In view of the low renal dose and the high tracer retention within the metastatic lesions, the delivered tumor dose is expectedly high and multiple therapies would be possible in this patient without undue concern for renal toxicity.

A recent study simulated the effect of an increase in PSMA-avid tumor volume to the tumor and renal dose using the data of 13 patients treated with 177Lu PSMA I&T.1 According to the simulation, a 10-fold increase in total tumor volume (0.3 L to 3 L) was associated with a reduction of mean renal absorbed dose from 6.5 Gy to 3.7 Gy: a decrease of slightly less than 50%. The conclusion of this study demonstrates that in patients with large PSMA-positive tumor volumes, higher activities can be safely administered to maximize tumor dose without exceeding maximum dose thresholds to critical organs. Dosimetry was performed using sequential planar scintigraphy in the referenced study. In comparison, the present case example utilizes xSPECT Quant with high accuracy of calculated tracer concentration along with dosimetry software, which enables automated segmentation of critical organs. A low level of renal cortical absorbed dose (3.6 Gy to the right kidney) therefore suggests the potential of multiple therapies in order to achieve higher tumor dose without crossing the renal absorbed dose threshold of 23 Gy. Since the patient has normal renal cortical thickness with absence of pelvicalyceal stasis, there is also the possibility of accepting a higher renal cortical dose threshold of 40 Gy, which would enable a significantly higher therapeutic window.


Using sequential quantitative SPECT/CT, based on calibration using a phantom with known concentration of 177Lu to enable conversion of counts to tracer concentration, a study evaluated renal absorbed dose in five patients with metastatic castration-resistant prostate cancer treated with two cycles (approximately 3.6 GBq each cycle) of 177Lu PSMA therapy.2 A mean renal absorbed dose was 2.2 Gy +/- 0.6 Gy. 3D volumes of the kidney, generated from sequential SPECT/CT images, were used to calculate total tracer concentration and generate timeactivity curves for dose estimation using tracer-specific S values. All patients showed overlap of intestinal and liver activity with the kidney on planar images, which was eliminated using SPECT/CT data, therefore the authors categorically recommended utiliizing 3D SPECT/CT-based dosimetry for all 177Lu PSMA studies to avoid this issue with planar scintigraphy. The present case example shows renal dose even lower than the study by Delker et al. with a mean renal cortical dose as low as 0.4 Gy/GBq (right kidney).
Tumor tracer concentration, as shown by xSPECT Quant, was high in the initial study with progressive increase up to 24 hours after injection followed by slow washout with almost 50% of peak tracer concentration retained at 96 hours. This suggests longer tracer residence time within metastatic lesions and consequently higher tumor absorbed dose. Since the present dosimetry study was based on the first therapy, subsequent therapy administrations need to be similarly evaluated using sequential xSPECT Quant studies and dosimetry to determine change in renal and tumor dose with respect to change in overall tumor burden.
Conclusion
Sequential xSPECT Quant studies following therapeutic dose of 177Lu PSMA enables 3D voxel-based dosimetry in a patient with multiple skeletal metastases from prostate cancer, which show normal renal cortical dose with high tumor retention of tracer.