
History
A 60-year-old female patient with severe obesity (300 kg body weight) was admitted to the hospital due to widespread erysipelas in her left leg, sepsis with streptococcus and acute renal failure. Her medical history included Levaxin-substituted hypothyroidism and psoriasis. After treatment, her renal function was normalized with a serum creatinine value of 34 μmol/L, and she was generally feeling better. A lung X-ray was performed and revealed a round, well-defined lesion, measuring 23 mm in diameter, at the level of the right pulmonary hilus with an unclear nature. Contrast enhanced chest and abdominal CTs were requested for further investigation.
Diagnosis
CT images showed a small, well-defined round lesion, 17 mm in diameter and without contrast enhancement in the right middle lobe. Further, there was a segmental atelectasis of the right lower lobe. No signs of bronchial obstruction were evident. With the side finding of a single gallbladder stone, the rest of the scan was unremarkable. The appearance of the lung lesion was regarded as benign.

Courtesy of Center for Medical Image Science and Visualization (CMIV), Medical Faculty/Radiology, Linköping University, Linköping, Sweden
Fig. 1: Axial images (0.5 mm) show a small, well-defined round lesion, without contrast enhancement, in the right middle lobe (arrows). A segmental atelectasis is seen in the right lower lobe (dotted arrows).
Courtesy of Center for Medical Image Science and Visualization (CMIV), Medical Faculty/Radiology, Linköping University, Linköping, Sweden
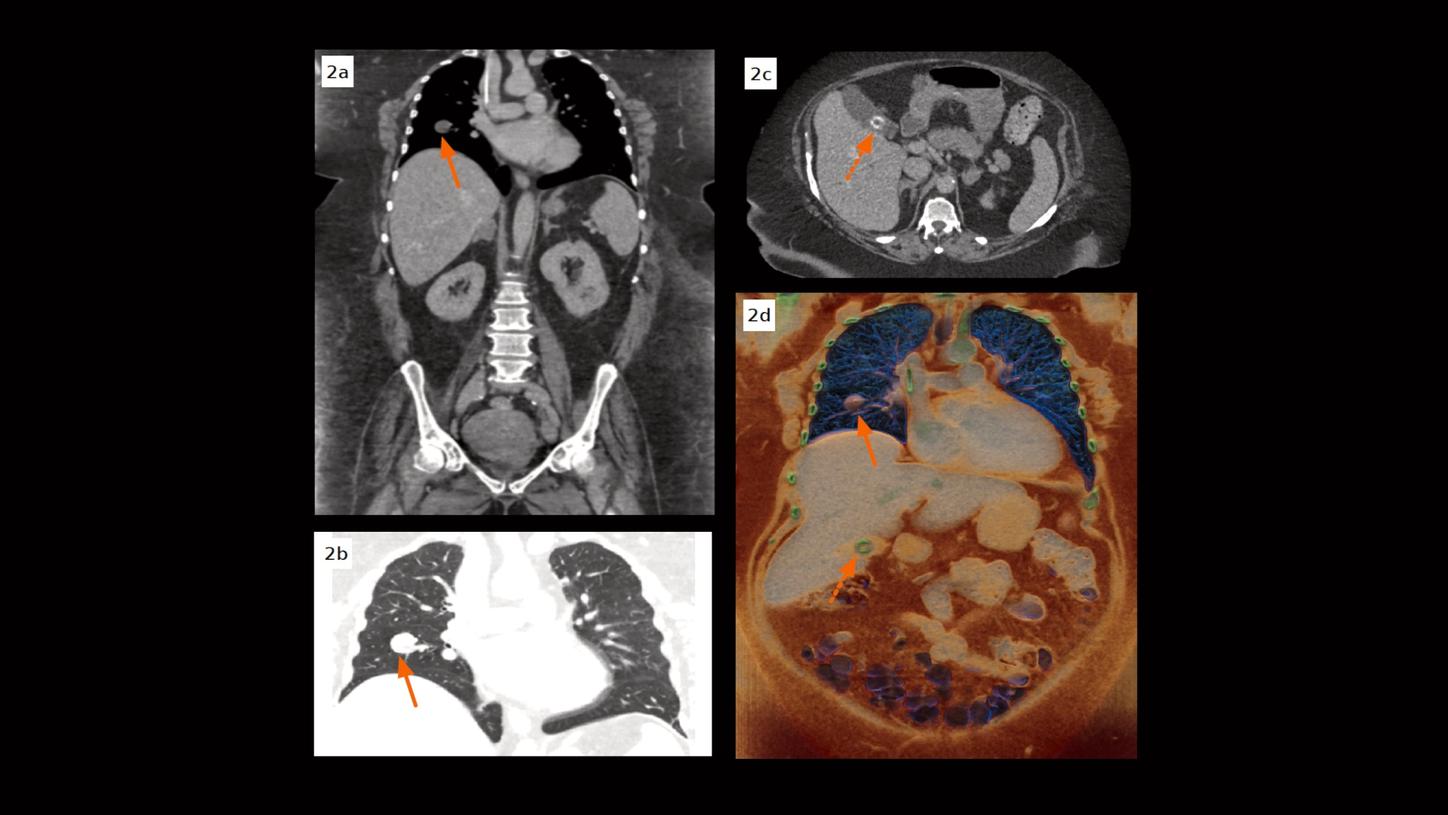
Fig. 2: Coronal MPR images (Figs. 2a & 2b, 0.5 mm) show a small, well-defined round lesion, without enhancement, in the right middle lobe (arrows). A centimeter-sized round gallstone with a hyperdense ring is seen in an axial image (Fig. 2c, dotted arrow). A cVRT image (Fig. 2d) reconstructed with 0.5 mm slices show both the lung lesion (arrow) and the gallstone (dotted arrow) in three dimensions.
Comments
The prevalence of obese and morbidly obese patients increases. [1] As image noise increases exponentially with increasing patient diameter due to greater photon attenuation and scattering, anatomical conspicuity in pertinent pathologic conditions is correspondingly decreased. This causes difficulties in image interpretation and may lead to repeated radiological or further clinical examinations, resulting in higher cumulative radiation dose and increased costs. If only considering the statistical noise of X-rays, the dose needs to be quadrupled to halve the image noise. The situation is even worse with the presence of substantial electronic noise. Therefore, image noise reduction comes at the cost of increased radiation dose which requires higher power output of the X-ray tube. The classical way of maximizing X-ray flux and tube output is lowering the pitch and increasing the rotation time; these measures, however, slow down the scan speed and increase breath-hold time with inherently increased presence of motion artifacts. Hence, despite all the advances made in conventional detector CT in recent years, obese patients are still a difficult target group for CT.
This case was performed on a NAEOTOM Alpha, a newly developed dual source CT scanner with photon-counting detectors (QuantaMax™), providing energy-resolved CT data without electronic noise. [2] Electronic noise is eliminated by setting up a predefined digital threshold for counting X-ray photons far above the electronic noise floor, leading to less image noise and, potentially, to the reduction of radiation dose. As electronic noise is dominant at low X-ray flux at the detector, such as in the case of a low dose or bariatric CT scan, its absence has a particular impact on the improvement of the image quality. Another important advancement is the higher contrast-to-noise ratio (CNR) in iodine contrast enhanced CT scans, due to the absence of down-weighting of lower energy X-ray photons. In the image reconstruction process, a model based iterative reconstruction approach – Quantum Iterative Reconstruction (QIR) – is applied for further image noise reduction. All of these improvements contribute to the reduction of image noise as well as radiation dose. For example – even slices as thin as 0.5 mm can be used for three-dimensional demonstration with great image details using cinematic volume rendering technique (cVRT). As presented in this case, although the patient weighs 300 kg, the CT scan required only 314 mA – less than one-third of the maximum power of a single X-ray tube (1,000 mA at 120 kV) – achieving optimal image quality that helped the physicians make a confident diagnosis.
Examination Protocol