History
A 53-year-old male patient, suffering from tiredness, nausea, vomiting and shortness of breath, presented himself to the emergency department. The patient had a known history of arterial hypertension. A CT angiography (CTA) was requested for evaluation.
Diagnosis
CTA images showed a saccular aneurysm at the aortic isthmus, beginning 0.6 cm distal to the left subclavian artery (LSA), measuring 6.1 cm in maximum diameter and extending over a distance of 4.4 cm. Neither calcified plaque nor mural thrombus were present. There were also no signs of extravasation of contrast media to suggest an impending rupture. The diameter of the aorta was measured both in front of (3.4 cm) and behind the aneurysm (3.6 cm). The origins of the innominate artery (IA), both common carotid arteries (CCA) and subclavian arteries (SA), as well as vertebral arteries (VA) appeared normal. No abnormalities were seen neither in the ascending nor in the descending aorta. The coronary arteries were normal with a right coronary artery (RCA) dominant system. The patient was referred to the vascular surgery department.

Courtesy of Department of Radiology, Beijing Electric Power Hospital, Beijing, P. R. China
Fig. 1: An axial image (Fig. 1a) and an oblique MPR image (Fig. 1b) show a saccular aneurysm (asterisk) at the aortic isthmus, beginning 0.6 cm distal to the LSA (arrows), measuring 6.1 cm in maximum diameter and extending over a distance of 4.4 cm.

Courtesy of Department of Radiology, Beijing Electric Power Hospital, Beijing, P. R. China
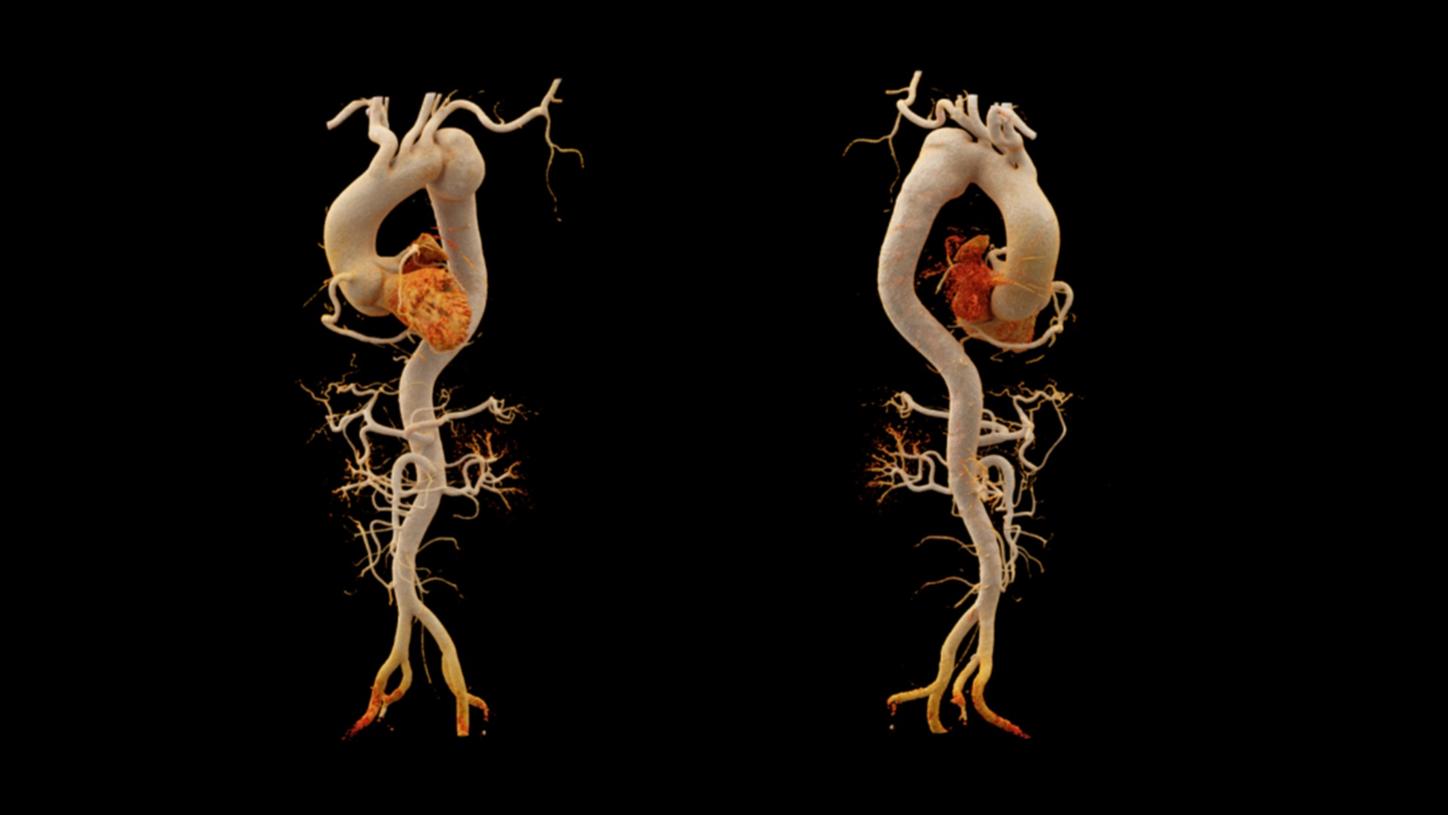
Fig. 2: cVRT images, with different presets, demonstrate three dimensional views of the aneurysm (arrows), the aorta and the coronary arteries.
Courtesy of Department of Radiology, Beijing Electric Power Hospital, Beijing, P. R. China
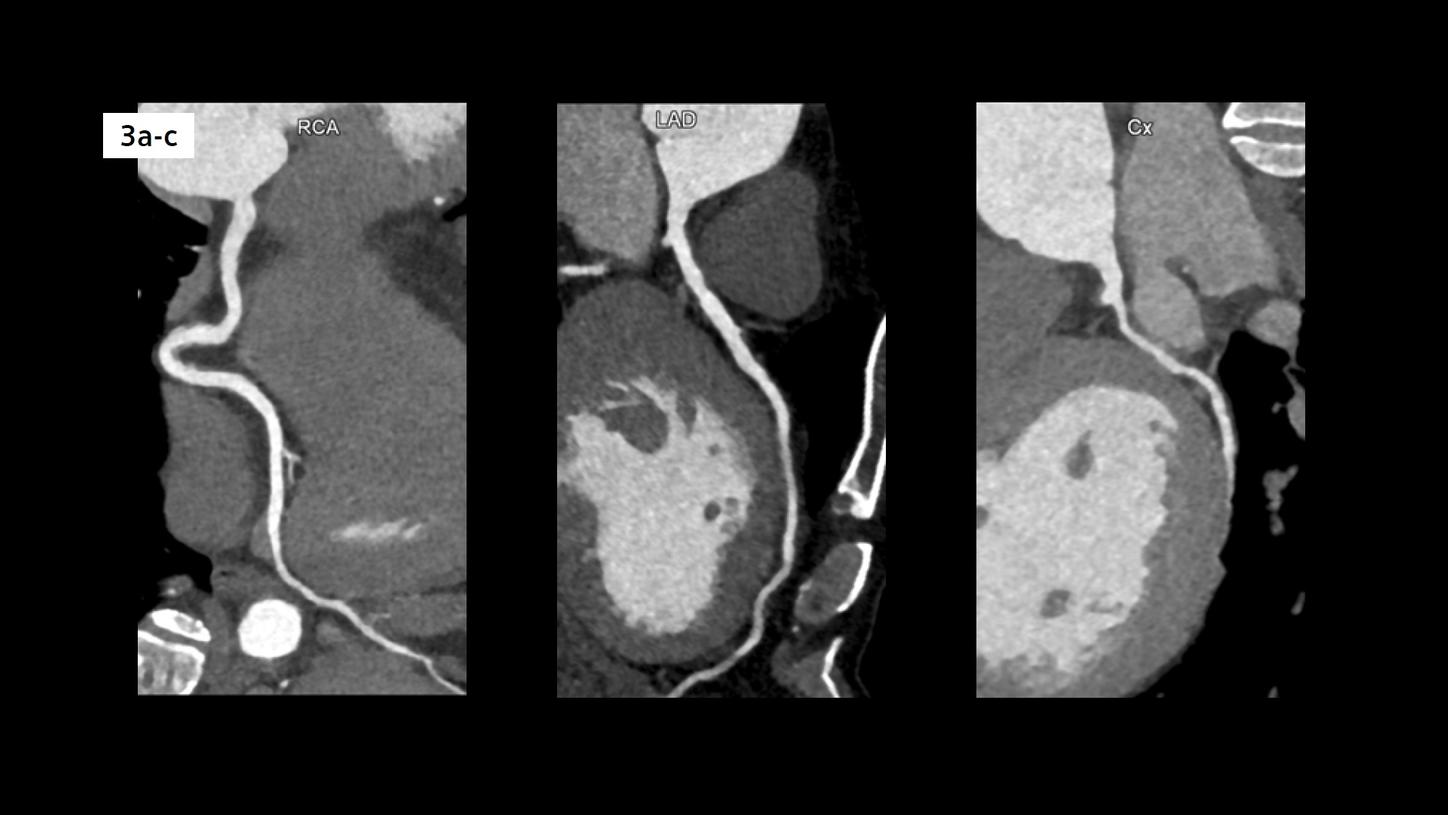
Fig. 3: Curved MPR images show three normal coronary arteries.
Comments
Thoracic aortic aneurysms involving isthmus are very rare. Most of these aneurysms are asymptomatic and slow-growing. They may go undiagnosed for a long period of time until they rupture causing sudden death. Saccular aneurysms, such as this case, appear to have an increased risk for rupture. Early diagnosis is therefore critical for patient management. CTA imaging clearly shows the location, size and extension of the aneurysm, providing confident diagnostic information. The challenge in this case is the fact that the patient could not cope with the breathing instructions due to his dyspnea. Therefore, a unique scanning technique, the Turbo Flash mode, is applied using a large pitch to obtain an ultrafast scanning speed. A range of 515 mm, covering the complete trunk, is acquired in just 1.1 s in free breathing. Optimal image quality, without motion artifacts, is achieved depicting the complete aorta, the aneurysm and the coronary arteries. A lower kV setting of 80 kV is applied to improve the contrast-to-noise ratio, reducing the radiation exposure and the amount of contrast agent needed. Standard dose reduction techniques, such as CARE Dose4D (automatic controlled tube current modulation) and ADMIRE (Advanced Modeled Iterative Reconstruction) are applied as well to reach a radiation dose level as low as 2.8 mGy. Image demonstration, using cinematic volume rendering technique (cVRT), provides a better 3D perspective with improved depth and shape perceptions, enabling a lifelike demonstration, and ultimately, facilitates communication with the patient and physicians.