SOMATOM go.Sim Together, creating efficiency
SOMATOM go.Sim allows a streamlined simulation process: Enhancing the patient experience, driving towards the reduction of risks within the complex RT simulation workflow, all with the intention of improving the workforce productivity.
Designed and developed considering the needs of the radiation therapy staff: We are together creating efficiency.

Benefits
Courtesy of Radiology Department, Hospital Particular de Viana do Castelo, Portugal.
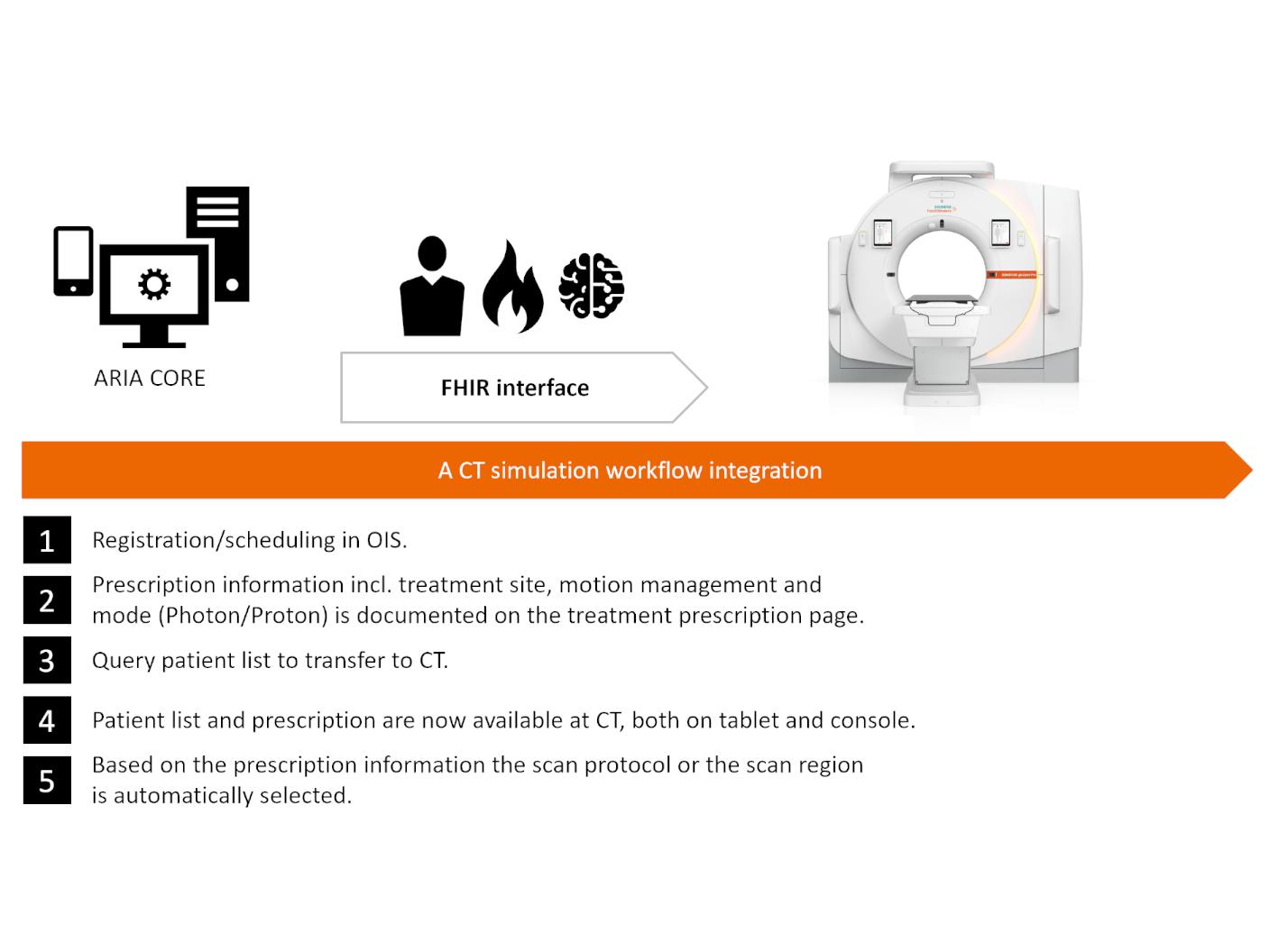
SOMATOM go.Sim provides a comprehensive solution tailored to maintain consistency across your simulation process. Its user-friendly interface, specialized RT workflow, and AI contouring support work seamlessly together to foster coherence during treatment planning.


Courtesy of Leopoldina Krankenhaus Schweinfurt, Germany

Evidence
Efficiency

Reduce complexity in the simulation process: Direct Laser and Direct Laser QA.
Direct Laser1
- Streamlined patient marking thanks to fully integrated lasers
- No need for separate laser hardware resulting in a smaller system footprint
- Direct Laser QA provides a quick quality assurance check with a dedicated phantom



Quality
 Without iMAR
Without iMAR With iMAR
With iMARCourtesy of Leopoldina Krankenhaus Schweinfurt, Germany
iMAR1 - iterative metal artifact reduction
- Optimized images for better tissue contrast
- Enhanced metal artifact reduction specifically adapted for different types of implants including:
- Thoracic coils
- Shoulder implants
- Hip implants
- Spine implants
- Extremity implants
- Pacemakers
- Neuro coils
- Dental fillings
Without iMARWith iMAR

Precision

DirectDensity1 guided by CARE kV empowers the use of optimized kV settings for each individual patient.
DirectDensity1,4
- Drive precision for target contouring with automatic and patient-specific, optimized kV imaging (CARE kV in 10 kV steps)
- Electron density and mass density reconstruction with DirectDensity1,4
- A standardized workflow with a single calibration curve for dose planning


Testimonials
"DirectORGANS is our first use of autocontouring. We can definitely see the benefits in terms of time saving. We feel it's very accurate most of the time, very little edits are needed to be made."6

Hull University Teaching Hospitals, NHS Trust, UK



Take a closer look at SOMATOM go.Sim

Technical Details
Bore size
85 cm
Scan Field-of-View (sFOV)
60 cm
Acquired slices/reconstruction slices
32/64
Z-axis coverage
1.92 cm
Rotation time
0.351, 0.5, 1.0 s
Max. table load
227/3071 kg (TG-66 compliant tables)
System footprint
4 m2/43 ft2 (surface area covered by gantry and moving table top)
Min. room requirement
17.3 m2/186.2 ft2
Related topics

CT simulation for Radiation Therapy
Imaging marks the beginning of a patient's RT treatment pathway. See why we believe that the very first image plays a curcial role throughout the whole treatment.

NAEOTOM Alpha.Prime RT Pro Edition
Count on clarity: clarity is where confident decisions begin. In radiation therapy, clarity reveals what matters, reduces uncertainty, and guides the path forward.

SOMATOM go.Open Pro
Together, moving ahead: Push your clinical boundaries and remain at the forefront of imaging in RT.
