
1Department of Radiology, Herlev and Gentofte Hospital, University of Copenhagen, Denmark;
2Siemens Healthineers, Denmark;
3Department of Radiology, Frederiksberg and Bispebjerg Hospital, University of Copenhagen, Denmark
History
A 23-year-old male patient, presented himself to the emergency department one day after a fall from a bicycle onto his left wrist. At initial presentation, the patient had no pain at rest, but complained when pressure was applied over the scaphoid bone (snuffbox tenderness). Radiographs, with scaphoid-specific projections, were taken but no fractures were demonstrated. Due to clinical suspicion of a radiographically occult scaphoid fracture, the patient was referred to a Dual Energy CT (DECT) scan of the wrist.
Diagnosis
DECT images revealed bone marrow edema (BME) and an undislocated fracture through the waist of the scaphoid bone. The scapholunate distance was normal. No fractures in other wrist bones were seen. CT findings were subsequently confirmed by MRI (1.5T), performed the same day. The patient was treated with immobilization in cast for 6 weeks. Follow-up imaging after 8 weeks, showed signs of healing and ruled out non-union.


Courtesy of Herlev and Gentofte Hospital, Frederiksberg and Bispebjerg Hospital, University of Copenhagen, Denmark


Fig. 1: Sagittal reformats from MRI T1w 3D sequence (Fig. 1a), conventional CT (Fig. 1b) and DECT color-coded VNCa (Fig. 1c). BME (arrows) through the waist of the scaphoid is clearly shown in both MRI and DECT. The fracture is not visible in conventional CT.
Comments
Missed scaphoid fractures on radiographs are a concern, as untreated scaphoid fractures can lead to non-union.[1] Up to 40% of patients with clinical signs of a scaphoid fracture with negative radiographs have a scaphoid or distal radius fractures.[2] Therefore, patients with wrist trauma routinely undergo MRI or CT examinations. Both modalities have a high specificity for the detection of scaphoid fractures, however, CT had a lower sensitivity than MRI. This is, in part, due to the fact that a conventional CT couldn’t detect BME and failed to detect trabecular fractures.[3–5]
DECT
scans with virtual non-calcium (VNCa) applications were recently introduced to
our institution, allowing us to diagnose patients suspected of wrist fractures
with negative radiographs. The application allows calculation of the calcium
content and reconstruction of VNCa images demonstrating bone marrow edema. The
VNCa images are reconstructed in syngo.via (VB20, Resolution 1, Maximum
1,500 HU, Threshold -300 HU) and visualised with a color look-up table (atomic
number, window level 0 HU, window width 300 HU) at 2 mm slab thickness. Due to
the novelty of the examination technique, patients subsequently undergo MRI as
well.
A recent study [6] demonstrated the ability of DECT scans to show such occult fractures with a diagnostic accuracy similar to MRI. Due to the short duration of the DECT examination (approx. 1 minute in scanner), it offers logistical advantages over MRI.
In this patient, the undislocated scaphoid fracture was difficult to visualize in the conventional CT images alone, but the fracture associated bone marrow edema was clearly visible in the DECT VNCa images, allowing the physicians to make a confident diagnosis.

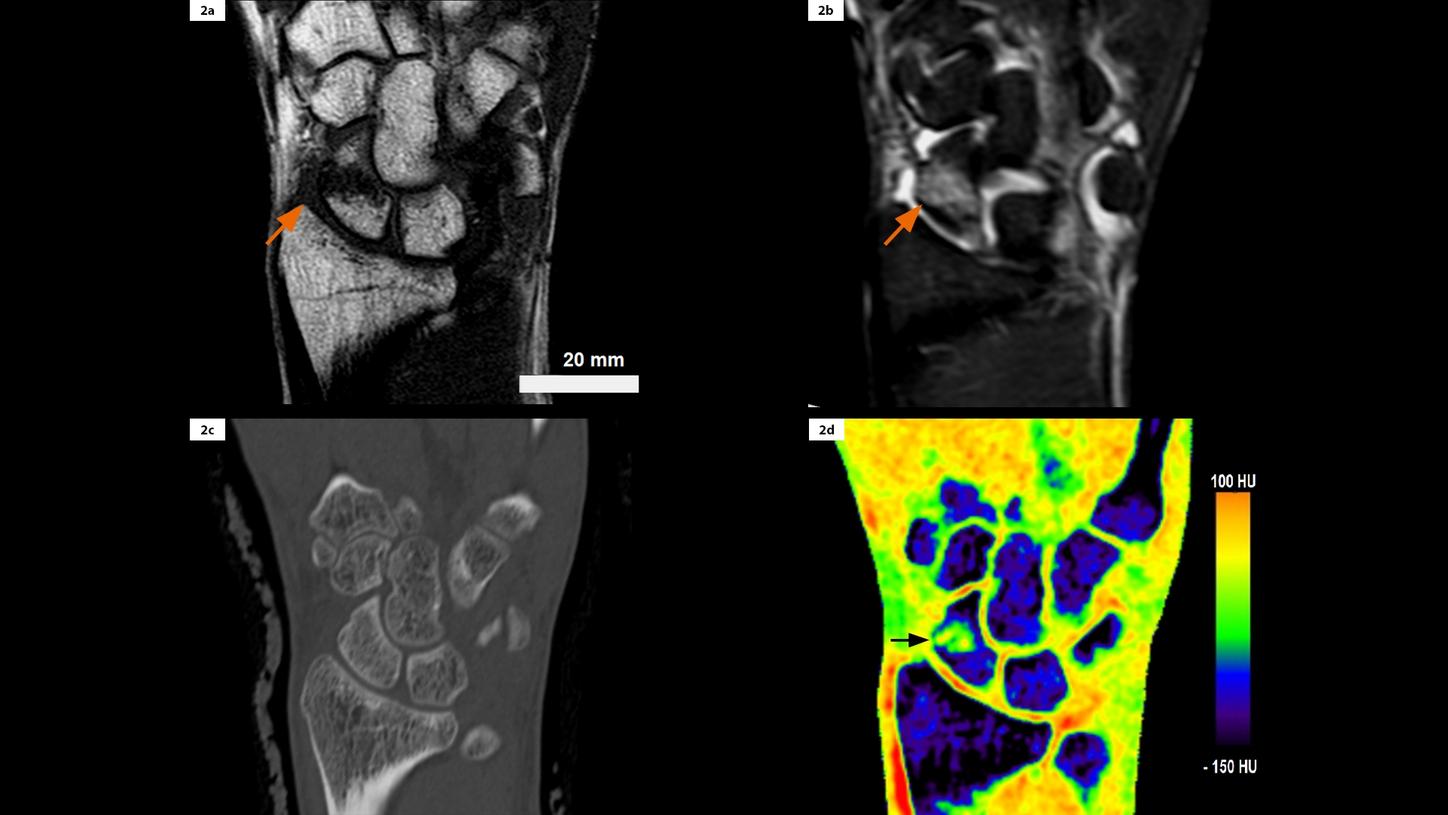
Courtesy of Herlev and Gentofte Hospital, Frederiksberg and Bispebjerg Hospital, University of Copenhagen, Denmark



Fig. 2: Coronal reformats from MRI T1w (Fig. 2a), MRI STIR (Fig. 2b), conventional CT (Fig. 2c) and DECT color-coded VNCa (Fig. 2d). BME (arrows) through the waist of the scaphoid is clearly shown in both MRI and DECT. The fracture is not visible in conventional CT.