Abstract
The recent implementation of the Siemens Healthineers NAEOTOM Alpha photon-counting computed tomography (PCCT) system at Sengkang General Hospital (SKH) has significantly advanced the diagnostic capabilities of coronary computed tomography angiography (CCTA), particularly in patients with elevated coronary artery calcium (CAC) scores. This article explores the clinical benefit of reduced blooming artefact enabled by PCCT technology and outlines a paradigm shift in departmental practice - specifically, the removal of the historical calcium score cutoff for CCTA eligibility.
Introduction
Coronary CT angiography has become a cornerstone in the non-invasive assessment of coronary artery disease (CAD). However, in patients with high CAC scores (typically >1000), the diagnostic accuracy of CCTA is often compromised due to blooming artefact, which can obscure the true lumen and lead to overestimation of stenosis or non-diagnostic segments. Historically, SKH and many institutions imposed a CAC score threshold above which patients would be triaged directly to invasive angiography or alternative imaging modalities.
Photon-counting CT, introduced clinically via the NAEOTOM Alpha, offers revolutionary detector technology that enables higher spatial resolution, reduced noise, and more precise material decomposition capabilities. This article presents SKH’s initial clinical experience with PCCT, demonstrating markedly improved visualization of the coronary arteries in patients with heavy calcification and justifying the removal of the calcium score exclusion criteria for CCTA.
Technological Background
Photon-counting CT differs fundamentally from conventional energy-integrating detector CT systems. By counting individual X-ray photons and classifying them into energy bins, PCCT eliminates electronic noise and significantly improves spatial resolution and contrast-to-noise ratio. This is particularly beneficial in vascular imaging, where vessel wall calcifications traditionally introduce artefacts that obscure vessel lumen assessment.
Key benefits include:
- Higher spatial resolution (~0.2 mm)
- Reduced blooming and beam hardening artefacts
- Improved calcium quantification and plaque characterization
Clinical Implementation at Sengkang General Hospital
SKH adopted the NAEOTOM Alpha in late 2024 with an initial focus on its potential to overcome limitations in cardiovascular CT imaging. A multidisciplinary review led to the adjustment of CCTA referral criteria. Previously, patients with CAC scores >1000 were generally excluded from CCTA, based on the high likelihood of inaccurate luminal assessment due to blooming.
Post-NAEOTOM Alpha Implementation:
- The calcium score cutoff was removed.
- All patients, regardless of CAC score, are now eligible for CCTA if clinically indicated.
- Radiologists report increased diagnostic confidence even in patients with CAC scores exceeding 6000.
Case Series and Observations
Illustrative Case Example:
A 48-year-old male with a CAC score of 6889 underwent CCTA using PCCT. Despite the high calcium score in the RCA, the RCA was shown to have minimal-mild stenoses. The LAD and LCX was shown to have moderate-severe stenoses.
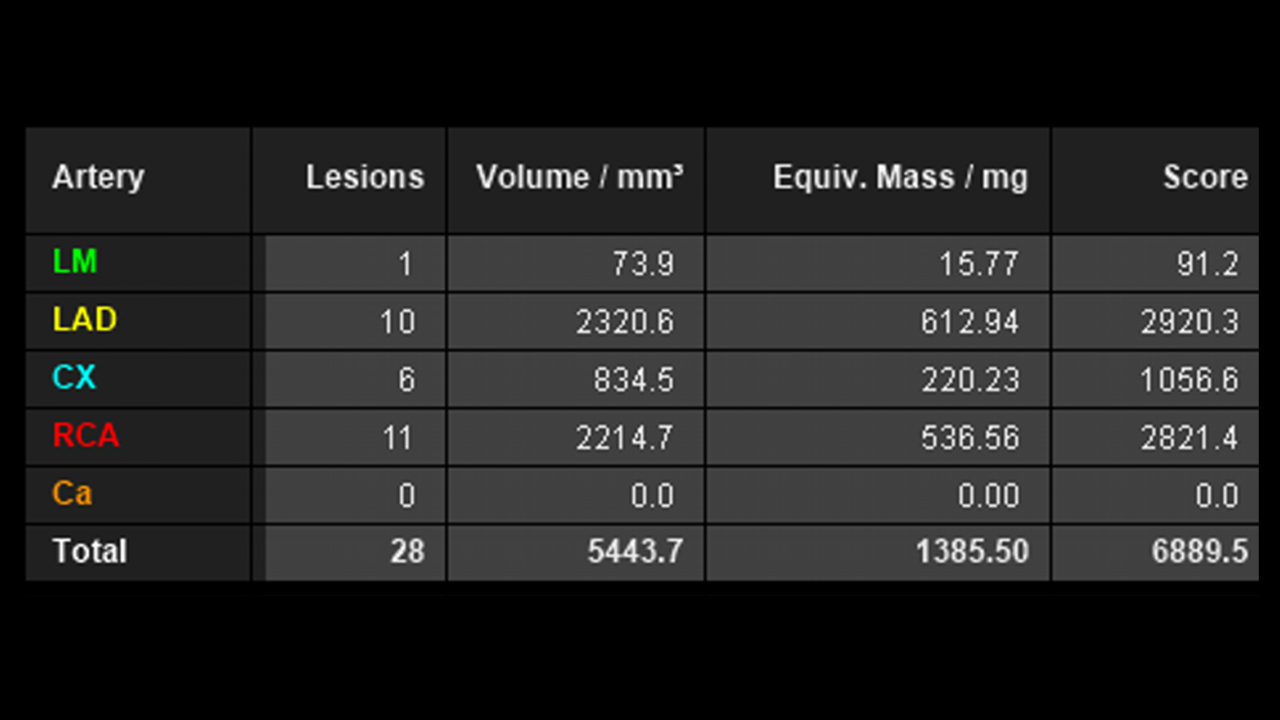
Coronary artery calcium (CAC) scores. Image courtesy from Sengkang General Hospital
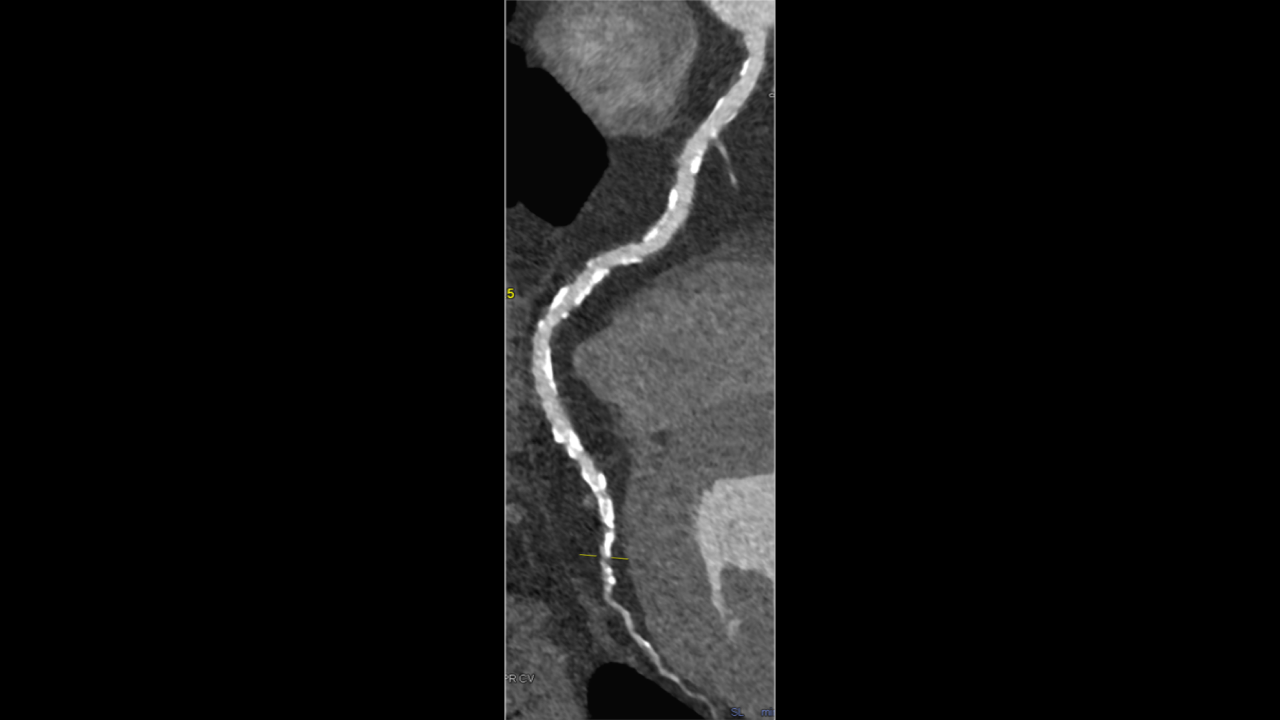
Image of the right coronary artery (RCA) showing non-obstructive disease. Image courtesy from Sengkang General Hospital
Discussion
Whilst this case showed areas of moderate-severe stenoses in the LAD and LCX requiring subsequent PCI. the RCA findings provides a good example of potentially right-siting patients and avoiding catheter angiography with the use of PCCT. This has been supported with previous publications as referenced.
The shift to photon-counting CT has enabled a transformative change in practice. By reliably visualizing coronary arteries in the presence of heavy calcification, PCCT has strengthened the role of CCTA as the viable and non-invasive option for cardiac vascular assessment even in patients with high or extreme CAC scores.
The reduced need for invasive angiography not only benefits patient safety but also alleviates resource strain in a high-volume public hospital setting. Radiologists also report improved inter-reader agreement and confidence in interpretation.
Conclusion
The integration of photon-counting CT via the NAEOTOM Alpha at Sengkang General Hospital has yielded a significant clinical advantage: the ability to perform accurate CCTA in patients previously deemed unsuitable due to high calcium scores. The resulting change in departmental policy to eliminate the CAC score threshold for CCTA reflects a growing recognition of PCCT's potential to redefine coronary imaging standards and allow for non-invasive assessment of a larger group of patients who would previously have had only invasive options available for accurate diagnosis.
Written by

Dr Tan Min On is a Consultant Chest, Cardiac and Body Radiologist at Sengkang General Hospital. He has deep interest in quantitative imaging and artificial intelligence applications.

Dr Srujana Ganti is Consultant Radiologist and is the lead for Cardiothoracic imaging services at Sengkang General Hospital. She has a particular interest in Cardiac and Lung Cancer Imaging.