Faecal Immunochemical Testing (FIT)The Power of Integration
Colorectal cancer (CRC) screening saves lives – especially when it is easy for patients and scalable for laboratories. Faecal immunochemical testing (FIT) supports population screening by enabling non-invasive, at-home sample collection and targeted referral to colonoscopy when results are positive. The Atellica CH Sentinel FIT Alliance Application – using the Sentinel Diagnostics FOB Gold® Tube Screen – can help laboratories meet growing screening demand with direct tube loading, optional hands-free auto-decapping on Atellica Solution with Atellica Integrated Automation, and efficient integration of automated FIT testing into routine chemistry workflows. population

Benefits
In 2022, the European Health Union announced a target of 90 percent of the EU population eligible for colorectal cancer (CRC) screenings be offered such testing by 2025.1 CRC occurs in the tissues of the colon and the rectum (Figure 1) and is the second leading cause of death from cancer in Europe.2 Early identification is associated with a high rate of treatment success.3
Screening programs can lower CRC disease burden, including increased detection and improved outcomes, especially when conducted in targeted populations.3-5 Data indicate countries with long-standing population screening programs achieve a meaningful reduction in CRC incidence over time.3

FIT uses a single stool sample, requires no dietary preparation, and is generally simpler for patients than older guaiac-based FOB tests – supporting higher screening uptake.

Screening with FIT helps identify disease (and potential bleeding from large precancerous polyps) earlier, when treatment success is typically higher.

Positive FIT results can be triaged to colonoscopy for diagnosis, which can reduce unnecessary colonoscopies and help prioritise higher-risk patients.

FIT on Atellica CH is suitable for high-volume screening programs, and can be integrated into routine laboratory workflows (including automated, high-throughput testing), improving efficiency and turnaround time.
FIT uses a single stool sample, requires no dietary preparation, and is generally simpler for patients than older guaiac-based FOB tests – supporting higher screening uptake.
FIT Testing
Initial testing for CRC typically falls into two categories:
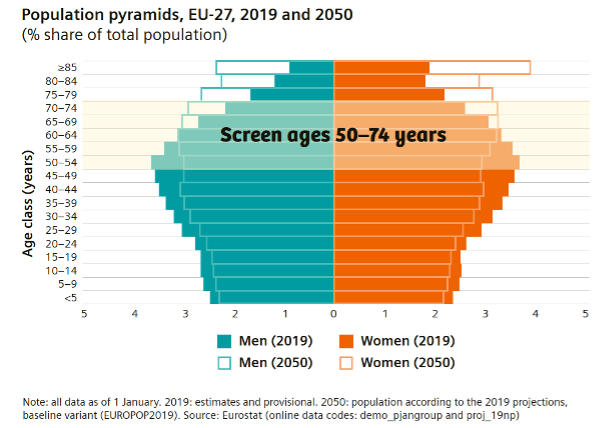
Screening in asymptomatic individuals is essential to improved detection, especially as early and more treatable forms often lack signs or symptoms (or may go unrecognised).7 Currently, the EU recommends CRC screening for all individuals aged 50–74 years1 in addition to testing for patients who are symptomatic.6 The large number of tests needed to meet screening targets necessitates assays that are amenable to ease of sample collection for increased uptake and scalable efficient analysis.5
Screening methods for CRC
Screening techniques include non-invasive testing or invasive endoscopic procedures (e.g., colonoscopy). Non-invasive faecal tests that detect the presence of hidden (occult) blood in the stool, which could be a sign of bowel cancer or polyps (especially large precancerous polyps), are widely available.8,9 As blood in the stool is not specific to CRC, positive tests typically reflex to colonoscopy for diagnosis and confirmation.10
Colonoscopy is essential to diagnose or exclude cancer or to identify and remove polyps. While colonoscopy also performs well as a screening test, it has several limitations for use in a high-volume testing population.12
Healthcare economic impact of screening
Prevention or early treatment of CRC is projected to have a substantial impact on healthcare costs.17-20 Early treatment of CRC is typically less costly while offering an improved quality of life and reducing deaths from CRC. In Europe, the estimated yearly economic burden of colon cancer is >19 billion euros, including ~ten-fold average increase in the cost of treating late vs. early-stage CRC.18 Broad uptake of screening recommendations could increase the percent of early cases diagnosed, saving an estimated 130,000 more lives, and producing 3 billion in healthcare savings each year.19 While testing frequency can impact costs, analysis indicates that even frequent (yearly) screening for CRC could be cost-effective and save more lives throughout Europe if widely implemented in targeted populations.20
Simplified collection and fully automated high throughput testing with the Atellica CH Sentinel FIT Alliance Application
While non-invasive, barriers to both gFOB and FIT testing can include the requirement for a stool sample collection, as well as concerns associated with laboratory operator exposure to the faecal material (especially when manually decapping). While FIT testing has generally simplified collection compared to gFOB, methodology (sample tube and testing modality) can vary between manufacturers.

Now, through an alliance with SENTINEL Diagnostics and Siemens Healthineers, FIT samples can be readily collected by the patient using the Sentinel Diagnostics FOB Gold® Tube Screen and analysed on the Atellica CH 930 Analyser or fully automated with decapping on the Atellica Solution with Atellica Integrated Automation.23
Operator exposure to the sample is minimised through the programmed auto-decapping of the Sentinel Diagnostics FOB Gold Tube Screen. This partnership mitigates many of the drawbacks associated with a user-defined method, as the Sentinel FIT alliance application on the Atellica CH 930 analyser is fully validated and supported by Siemens Healthineers.
Use of an existing Atellica Solution with Atellica Integrated Automation eliminates the need for additional specialised equipment, minimises operator risk of sample exposure, and fully integrates automated FIT testing into routine chemistry workflow.
“Hands-free” FIT testing on Atellica Solution with Atellica Integrated Automation
Routine FIT testing using the FOB Gold Tube Screen sample collection tube can now be fully automated on existing equipment (Atellica CH 930 analyser or Atellica Solution with Atellica Integrated Automation) used for chemistry testing in labs
Technical Details
Benefits of FIT testing using FOB Gold patient collection tube on the Atellica Portfolio
Sample collection
Sample Transport
The patented 2-in-1 sample collection-dilution tube offers an easy to use, hygienic, and non-invasive solution for at-home sample collection.† With just a single sample required and no patient pre-preparation provides a
seamless and private experience for the patients. Data indicate ease of patient collection is similar or superior to other commonly used FIT methods.*
By dissolving and diluting the patient sample in the buffer solution upon re-insertion of the collection stick, the process ensures the sample is properly prepared for easy and efficient transport to the testing site.
The patented design of the patient collection tube ensures consistent sample volume,† optimising accuracy and reliability for analytical testing.
The patient collection tube extracts and preserves haemoglobin from the stool sample, ensuring its stability across a broad temperature range, allowing for accurate testing upon transport to the laboratory.‡
Evidence
FIT cut‑point selection
FIT performance varies by the cut‑point selected, and laboratories should establish cut‑off values based on the assay used and the population tested. Colonoscopy referral rates and CRC detection differ between assays and cut‑points; however, good performance has been demonstrated across a range of quantitative FIT assays in diverse screening populations.
While no FIT assay achieves 100% accuracy, studies using the Sentinel FOB Gold assay showed low incidence of CRC following a negative result and >80% CRC detection across all cut‑points evaluated, supporting its use in risk assessment. Individuals with a negative screening result should be retested at the recommended two‑year interval.
Lower cut‑points generally improve sensitivity at the expense of specificity, allowing laboratories to adjust thresholds to optimise referrals within their target population. Sensitivity may vary by cancer stage and tumour location, with lower detection rates reported for stage I cancers, a limitation shared by alternative screening methods.
“We observed a low cumulative incidence of interval CRCs because of a high FIT sensitivity for CRC.”
Early‑stage CRC detection
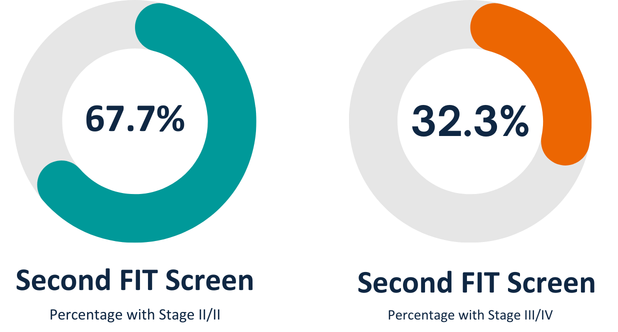
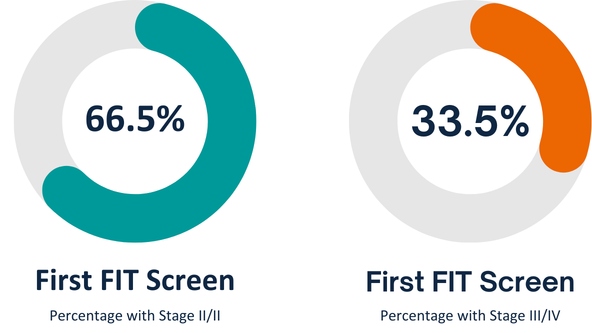
FIT screening is effective for detecting both early and late‑stage CRC. Studies using Sentinel FOB Gold showed most detected cancers were early stage (Stage I/II), with additional early‑stage detection achieved through repeat screening, reinforcing the importance of ongoing programs and appropriate cut‑point selection.
Screening programs recommend FIT testing and increase CRC detection leading to improved outcomes. Data shows testing with FIT may reduce colonoscopy burden and help prioritise those at higher risk. The ability to fully automate FIT testing on the widely available Atellica Solution and Atellica Solution with Atellica Integrated Automation supports the large number of tests mandated by screening programs and cancer reduction initiatives. Direct load and testing from the primary Sentinel FOB Gold sample collection tube without the need for cap removal minimises operator exposure and enhances workflow and the delivery of timely results.
Downloads
|
DownloadContact
Are you interested in finding out more on FIT Testing
Please contact us for more information
2. Fact Sheet, March 2024. Uncovering Inequalities Colorectal Cancer Screening in Europe. https://cancer-inequalities.jrc.ec.europa.eu/sites/default/files/ECIR-inequalities-factsheet-colorectal-cancer-screening-Mar2024.pdf
3. Cardoso, R. et al. Colorectal cancer incidence, mortality, and stage distribution in European countries in the colorectal cancer screening era: an international population-based study. The Lancet Oncology, Volume 22, Issue 7, 1002 – 1013
4. Blom, J. et al. Routine Fecal Occult Blood Screening and Colorectal Cancer Mortality in Sweden. JAMA Network Open. 2024;7(2): e240516)
5. Moss, S. et al. Increased uptake and improved outcomes of bowel cancer screening with a faecal immunochemical test: results from a pilot study within the national screening programme in England. Gut 2017; 66:1631-1644
6. Monahan KJ. et al. Faecal immunochemical testing (FIT) in patients with signs or symptoms of suspected colorectal cancer (CRC): a joint guideline from the Association of Coloproctology of Great Britain and Ireland (ACPGBI) and the British Society of Gastroenterology (BSG) Gut 2022; 71:1939–1962.
7. Larson, MB. et al. Effectiveness of Colorectal Cancer Screening in Detecting Earlier-Stage Disease—A Nationwide Cohort Study in Denmark. Gastroenterology 2018; 155:99–106
8. Song LL, Li YM. Current noninvasive tests for colorectal cancer screening: An overview of colorectal cancer screening tests. World J Gastrointest Oncol 2016; 8(11): 793800
9. Lauby-Secretan, B. et al. The IARC Perspective on Colorectal Cancer Screening. 2018; N Engl J Med 378;18 10. Zorzi M. et al. Non-compliance with colonoscopy after a positive faecal immunochemical test doubles the risk of dying from colorectal cancer. Gut 2022; 71:561–567
11. Shaukat, A. and Levin, T.R. Current and future colorectal cancer screening strategies. Nat Rev Gastroenterol Hepatol 19, 521–531 (2022)
12. Gimeno-García, AZ and Quintero, E. Role of colonoscopy in colorectal cancer screening: Available evidence. Best Practice & Research Clinical Gastroenterology 66 (2023) 101838
13. Grobbee, EJ et al. Guaiac-based faecal occult blood tests versus faecal immunochemical tests for colorectal cancer screening in average‐risk individuals. Cochrane Database Syst Rev. 2022 Jun 6;2022(6):CD009276
14. Hamza, S. et al. Diagnostic yield of a one sample immunochemical test at different cut-off values in an organised screening programme for colorectal cancer. European Journal of Cancer 49 (2013) 2727–2733
15. Martín-López, JE et al. Comparison of the accuracy of CT colonography and colonoscopy in the diagnosis of colorectal cancer. (2014) Colorectal Dis,
16: O82-O89.) 16. Anand S. and Liang PS. A Practical Overview of the Stool DNA Test for Colorectal Cancer Screening. Clin. Transl. Gastroenterol. 2022 Apr 1;13(4)
17. Ladabaum, U. et al. Cost-Effectiveness and National Effects of Initiating Colorectal Cancer Screening for Average-Risk Persons at Age 45 Years Instead of 50 Years. Gastroenterology 2019; 157:137–148
18. https://health.ec.europa.eu/system/files/2021-03/ev_20210303_js01_en_0.pdf
19. White paper. CRC screening in Europe. Saving lives and saving money. https://www.digestivecancers.eu/wp-content/uploads/2020/02/466-Document-DiCEWhitePaper2019.pdf
20. Pokharel R. et al. A Systematic Review of Cost-Effectiveness Analyses of Colorectal Cancer Screening in Europe: Have Studies Included Optimal Screening Intensities? Appl Health Econ Health Policy. 2023 Sep;21(5):701-717
21. Ola, I. et al. Utilization of colorectal cancer screening tests across European countries: a cross-sectional analysis of the European health interview survey 2018–2020. The Lancet Regional Health – Europe 2024;41: 100920
22. Li, SJ et al. Faecal immunochemical testing in bowel cancer screening: Estimating outcomes for different diagnostic policies. J Med Screen, 2021, Vol. 28(3) 277–285 23. FOB Gold® NG Wide Alliance Application Sheet. REF 1156009 CE. On file with Siemens Healthineers
24. https://www.who.int/news-room/fact-sheets/detail/colorectal-cancer#:~:text=Colorectal%20cancer%20is%20the%20third,when%20treatment%20options%20are%20limited Accessed January 21, 2025
25. Meklin, J. et al. Colorectal Cancer Screening with Traditional and New-generation Fecal Immunochemical Tests: A Critical Review of Fecal Occult Blood Tests. ANTICANCER RESEARCH 40: 575-581 (2020)
26. Vuik, FER. et al. Increasing incidence of colorectal cancer in young adults in Europe over the last 25 years. Gut, 2019;68:1820–1826