By Philipp Ritt, PhD, Torsten Kuwert, MD, Clinic of Nuclear Medicine, University Hospital Erlangen, Germany, and Partha Ghosh, MD, Siemens Healthineers, Hoffman Estates, IL, USA

History
An 82-year-old female patient with a history of thyroid cancer presented with multiple lung lesions detected on a chest CT, which were regarded as suspicious for metastases. Twenty years ago, the patient was diagnosed with primary thyroid carcinoma and underwent a near-total thyroidectomy and large-dose 131I therapy for ablation of residual thyroid tissue. She was treated with a total of 24 GBq of 131I and achieved complete ablation of the residual thyroid. Given the suspicion of lung metastases, diagnostic 131I scintigraphy was performed. A dosage of 597 MBq (16 mCi) of 131I was administered orally, and planar and SPECT/CT images were acquired 40 hours post-administration.
The study was performed on a Symbia Intevo™ 16 SPECT/CT using a high-energy collimator. Following the initial planar acquisition, a SPECT/CT study of the thorax was completed, with an initial CT acquisition (130kV, 40 eff mAs and 16 x 1.2 mm collimation) followed by a SPECT acquisition at 60 stops per detector and 21 seconds per stop, which resulted in 120 projections over 360°. Absolute quantification of 131I uptake was derived using xSPECT Quant™ [a], which is based on system calibration using a NIST-traceable 113Sn source. SPECT and CT data were fused, and lesion volumes and absolute tracer concentration were evaluated using syngo®.via.

Findings
Figure 1 notes multiple 131I-avid metastatic lesions in the lung and superior mediastinum on the planar whole-body image along with significant physiological retention of tracer in the stomach and a low level of tracer in the bladder and intestine. The SPECT and SPECT/CT images show a large metastatic lesion in the right lung base with a maximum dimension of 2 cm, along with several smaller metastatic lesions located in the right lung within the lateral aspect of the upper lobe, posterior paravertebral aspect of the left lung attached to the pleura, anterior aspect of the upper lobe of the left lung, and the anterior-superior mediastinum just below the sternum anterior to the trachea, which is likely a lymph nodal metastasis.
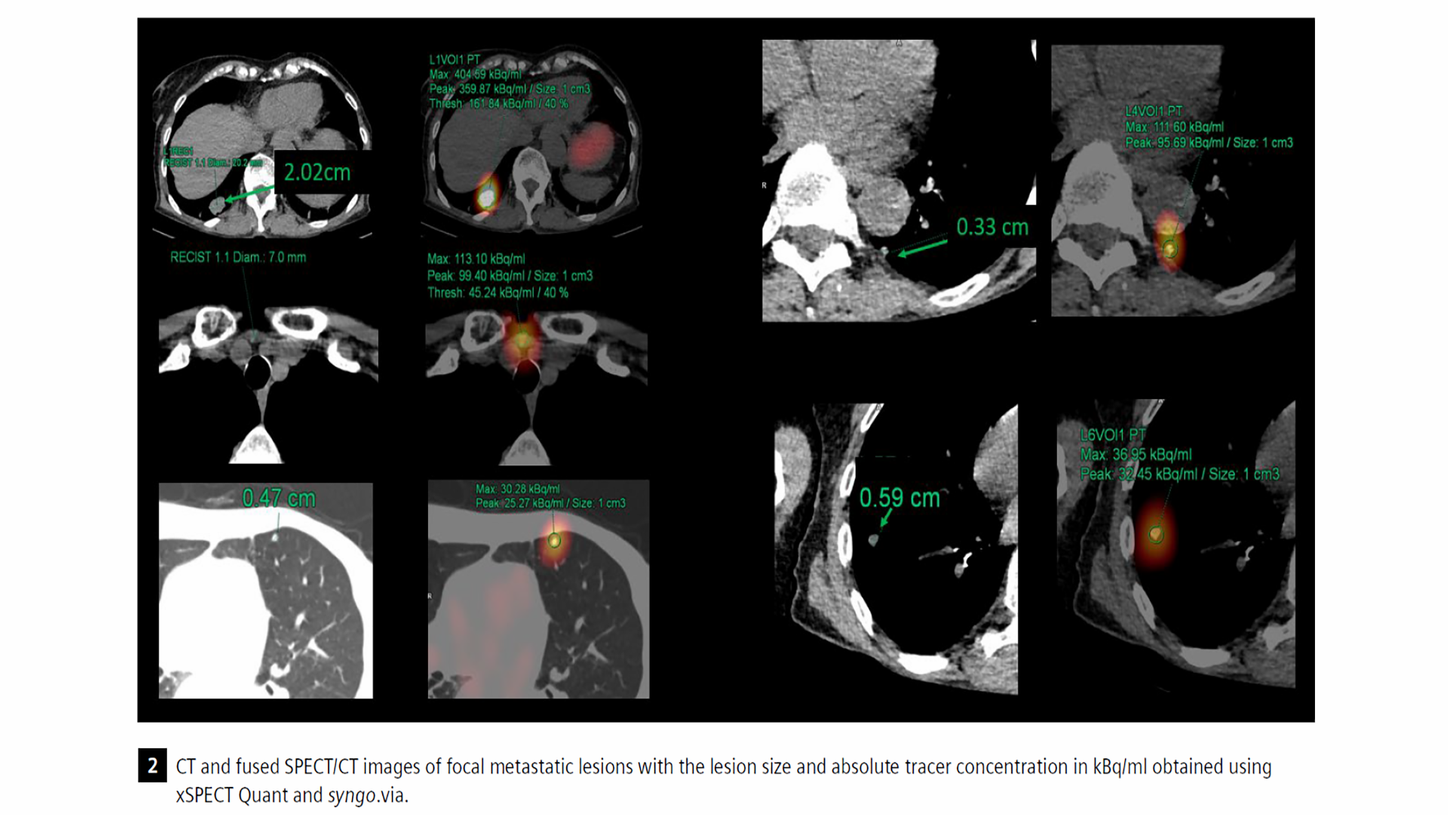
Figure 2 denotes the lesion size along with maximum and peak absolute concentration of tracer, which were obtained using 131I xSPECT Quant. The largest lesion, with a maximum dimension of 2 cm, shows a maximum concentration of 131I of 404 kBq/ml. The smallest lung metastasis, which is in the paravertebral space of the left lung attached to pleura (top left) and 3.3 mm in size, shows a lower maximum tracer concentration of 111 kBq/ml. A 6 mm lung nodule in the right lung (bottom right) shows maximum tracer concentration of 36 kBq/ml. The 5 mm lung nodule in the left upper lobe also showed similar maximum tracer concentration (bottom left). The increased intensity of tracer uptake in the small, 3 mm left lung metastasis, as compared to the 6 mm right lung metastases, is visually obvious in the planar as well as the SPECT images, and the absolute tracer concentration also correlates with the visual estimation, even though the lesion is small, which invites partial volume effects. The focal retrosternal nodal lesion in the anterior superior mediastinum also appears highly iodine-avid on both planar and SPECT, and the maximum absolute concentration of 113 kBq/ml reflects the visual impression. No bone lesions were seen on the SPECT/CT images. The single retrosternal nodal lesion also reflected high radioiodine avidity.
From this single-time-point, pre-therapy study following administration of a diagnostic dose of 131I, the number, size, and uptake intensity of lung and mediastinal lesions are well determined. The high uptake in the lung metastases, especially in the large metastases in the right lung base and the small lesion in the left lung attached to the pleura, suggests the possibility of high lesion-absorbed dose and a positive response following large-dose 131I therapy. However, in view of the need to predict the efficacy of large-dose 131I therapy and decide on the amount of 131I to be administered, the absorbed dose to lesions needs to be calculated from the quantitative values of the absolute tracer concentration, which are generated from the xSPECT Quant data along with the lesion volume estimation derived from CT.
Time-integrated activity coefficient was obtained by assuming a linear accumulation from administration until time of imaging (40 hours post administration), along with a mono-exponential decay with a half-life taken from literature. The time-integral activity curves (TIAC) were then multiplied with S-values extrapolated from the OLINDA solid-sphere model, which resulted in an absorbed dose in [Gy] and [Gy/GBq]. Activity in the lesions was taken from quantitative SPECT and segmented using an iso-contour (10% of maximum) in order to mitigate the impact of partial volume effect affecting the relatively small volumes of interest. The volumes of the lesions were determined from hand segmentation of the CT portion of the SPECT/CT acquisition.

Although sequential multi-time-point acquisitions are necessary to measure change in absolute tracer concentration within lesions in order to accurately calculate time-activity curves for absorbed dose estimations, in this patient, only a single time-point acquisition 40 hours post dose administration was available for dosimetry calculations. Thus, the half-life of the tracer within the metastatic lesions that was used for dosimetry was derived from published literature. Two half-life values of 48 hours and 67 hours noted as representing an acceptable range of half-lives1 were used to calculate a dose range for each metastatic lesion.
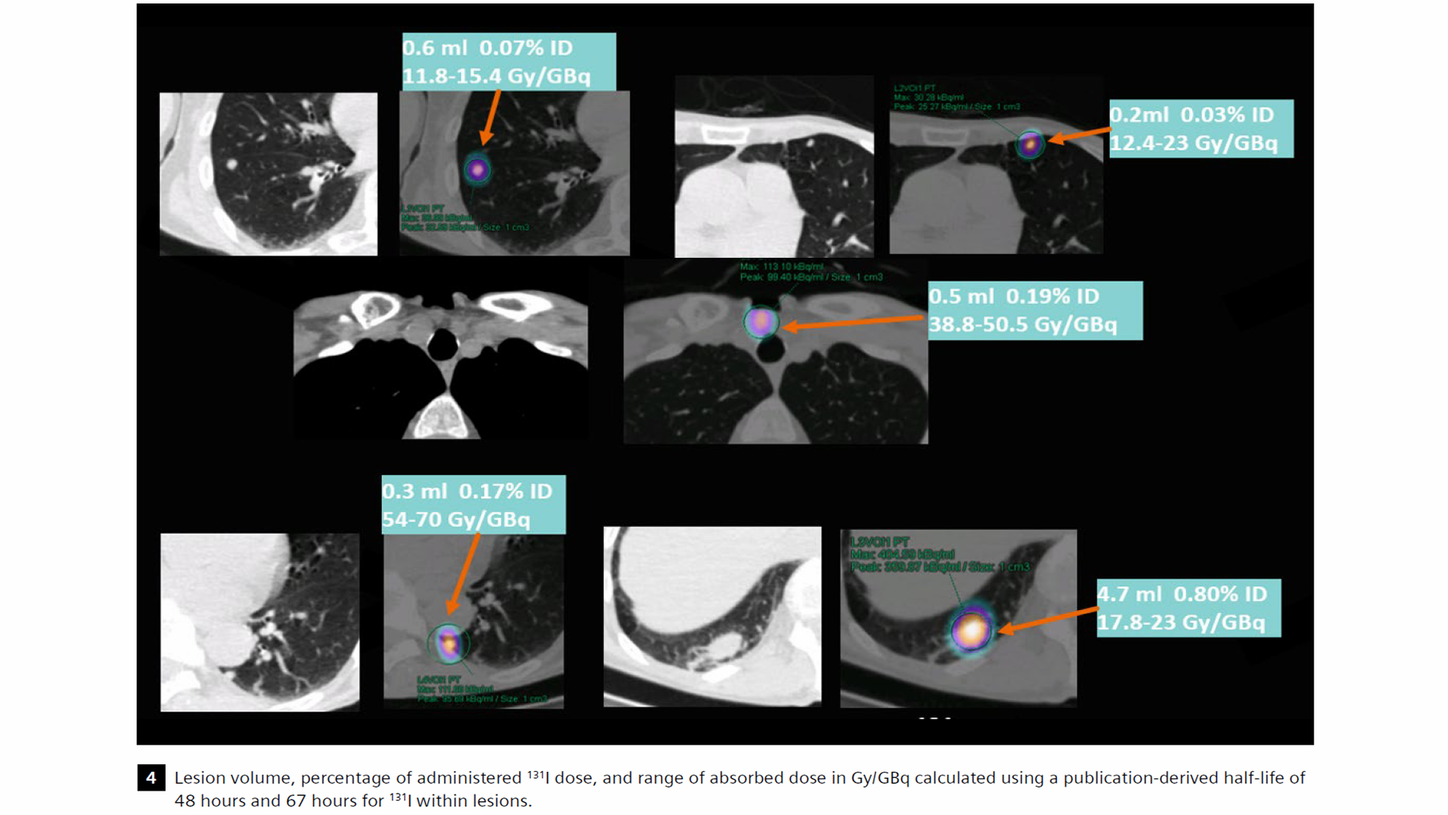
As Figure 4 shows, the largest lung metastasis with a volume of 4.7 ml and tracer retention of 0.8% of total administered dose was calculated to receive an absorbed dose of 17.8 Gy/GBq, if the half-life is considered to be 48 hours, and 23 Gy/GBq, if the half-life is considered to be 67 hours. For the small 0.3 ml paravertebral lesion attached to the pleura in the left lung with relatively high tracer concentration as shown on quantitative SPECT/CT, the absorbed dose ranges from 54-70 Gy/GBq, depending on the half-life considered. From the dosimetry calculations, it would require 4.34 GBq (approx. 110 mCi) of 131I to be able to deliver 100 Gy to the largest lung metastases considering 67 hours as half-life. Some of the smaller lesions may even be responsive to lower levels of administered activity.
Discussion
This case example illustrates the value of accurate estimation of absolute tracer concentration within lesions following diagnostic and post-therapeutic 131I administration in patients with metastatic thyroid carcinoma for absorbed dose calculation. Accurate volume estimation using diagnostic CT acquired as part of SPECT/CT and calculation of absorbed tracer concentration using xSPECT Quant based on system calibration using a NIST-traceable-113Sn source are key inputs for absorbed dose calculation. In this example, due to lack of sequential imaging, the effective half-life of the tracer within the lesions was based on a range (48 to 67 hours) obtained from literature and the time-activity curves derived from the absolute tracer and the accepted half-life range. These inputs were then used with OLINDA-based S-values to derive the range of absorbed dose for each lesion. Studies have shown that absorbed dose higher than 300 Gy to the residual thyroid tissue and 80 Gy to metastases are required for effective response: Maxon et al.2 demonstrated that 98% of tumors with an absorbed radiation dose of more than 80 Gy responded, while only 20% of tumors receiving less than 80 Gy showed significant response. A tumor dose <35 Gy was always associated with an absence of any response.
Pre-therapy dosimetry for a prediction of absorbed dose to critical organs and lesions following large dose 131I therapy was performed by Dorn et al3 with sequential whole-body planar acquisitions starting immediately after tracer administration and continued at daily intervals up to 4-5 days. The geometric mean of the anterior and posterior counts in multiple ROIs over lesions were used to generate time-activity curves, from which residence time and absorbed dose calculations were made. The objective of pre-therapy dosimetry was to enable the largest and safest dose without crossing the absorbed dose thresholds of 3 Gy for bone marrow and 30 Gy to the lungs.
Based on dosimetry studies, 41 therapy doses were delivered with curative intent since absorbed dose to metastatic lesions was calculated to be >100 Gy on pre-therapeutic dosimetry. Of these, 44% of patients could achieve >100 Gy tumor dose without crossing bone marrow or lung dose thresholds. The calculated dose to the metastases ranged from 100 Gy to >1,000 Gy. Most lesions receiving >100 Gy showed significant response on follow-up. Forty-six percent of patients had lowering of administered dose due to marrow and lung absorbed-dose estimations, which would have been higher than toxicity thresholds with doses required to achieve adequate tumor dose. There was a wide range of the administered 131I activity required to achieve a 3 Gy bone marrow dose (range: 7.4 GBq to 37.9 GBq) from the pre-therapy dosimetry. The authors concluded that higher initial 131I doses can be administered based on pre-therapy dosimetry in order to achieve significantly higher tumor-absorbed doses without exceeding critical-organ thresholds with significant tumor response whenever tumor-absorbed dose exceeded 100 Gy, as was seen in 44% of cases. No significant bone marrow or lung toxicity was seen in the entire patient group, reflecting the fact that pre-therapy dosimetry-based dose adjustment ensured no patient exceeded dose thresholds for these organs.
The calculation of absorbed dose based on a single-time-point quantitative SPECT/CT using literature-derived effective half-life of the tracer within lesions reflect a simplified approach to aid decision-making for large-dose 131I therapy in order to deliver adequate lesion dose. In this case, only the pretherapy scan performed with 16 mCi of 131I at 40 hours post administration was used for absorbed-dose estimation and predicted a dose of 110 mCi of 131I to deliver 100 Gy to the largest lung metastases. Although SPECT data at multiple time points would have been optimal for calculating the absorbed dose estimate, it was unfortunately not available in this case. Nevertheless, the calculations in this case were regarded as sufficient for guiding further therapy decisions. This approach could be easily extended to multiple-time-point scans. The accuracy of the quantification based on xSPECT Quant using a highly accurate NIST-traceable-113Sn source for system calibration together with attenuation correction using diagnostic CT as well as scatter correction is key to optimal dosimetry accuracy, which should be the major driver for therapy decision-making.
Conclusion
xSPECT Quant-based measurement of absolute concentration of 131I in thyroid carcinoma metastases in a patient who underwent a diagnostic 131I SPECT/CT study was instrumental in tumor-absorbed dose calculation based on literature-derived effective tracer half-life and helped guide further large-dose 131I therapy decisions.
Examination protocol
Scanner: Symbia Intevo 16