
Multiple Sclerosis – Diagnosis and follow-up with MRI
Multiple Sclerosis (MS) affects 1.8 million people worldwide, and every year 60,000 new patients are diagnosed with this autoimmune disease.1 MS results in damage to the myelin insulation of nerve cells, eventually leading to loss of transmission of nerve signals. As a consequence, a wide range of symptoms can be observed, from physical to mental and even psychiatric problems.
What MRI shows in MS patients
MRI is the imaging method of choice to support diagnosis of MS due to its variability in imaging contrasts. The following list provides an overview of the most relevant pathological indicators of MS and how MRI demonstrates these.
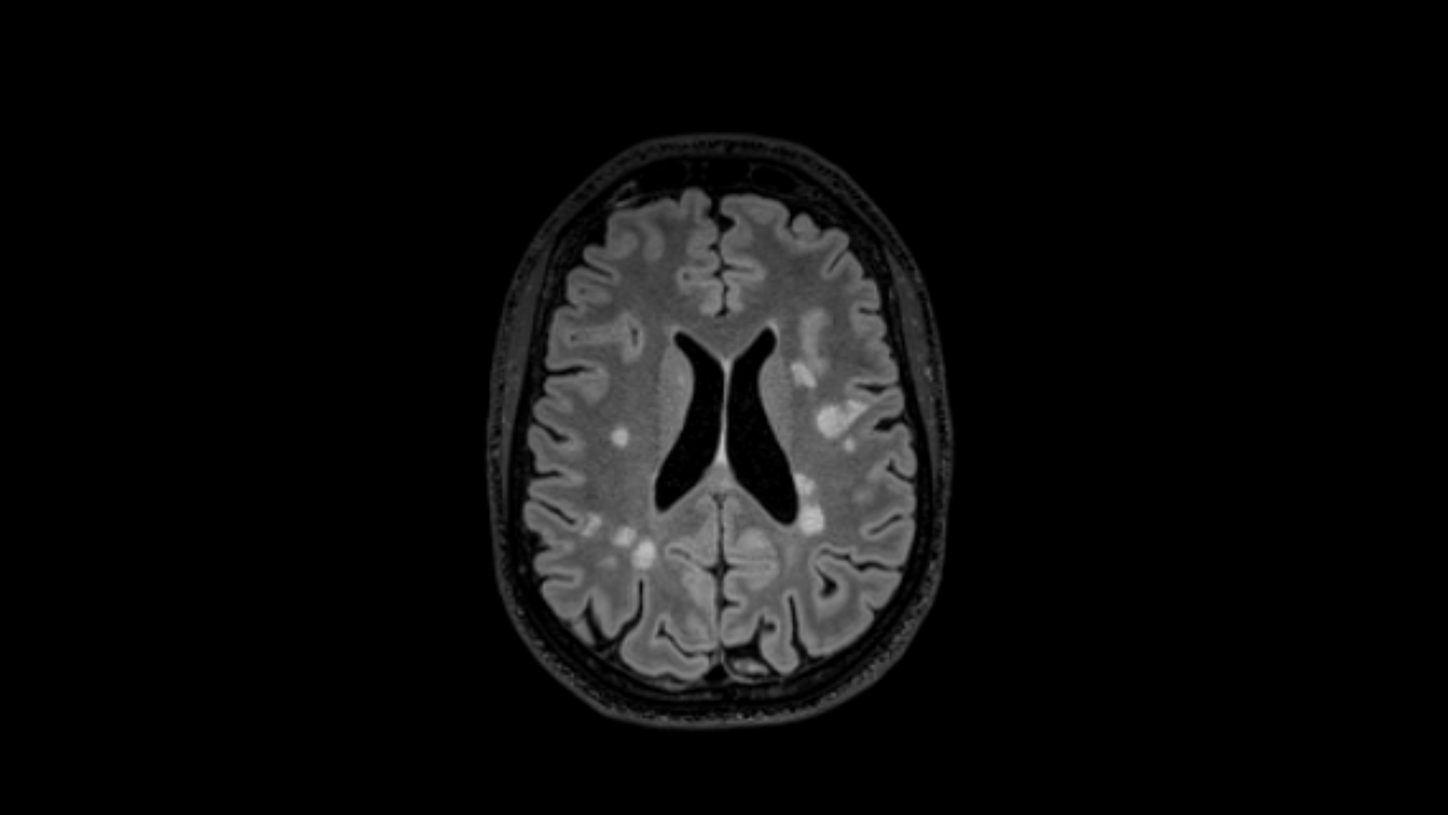
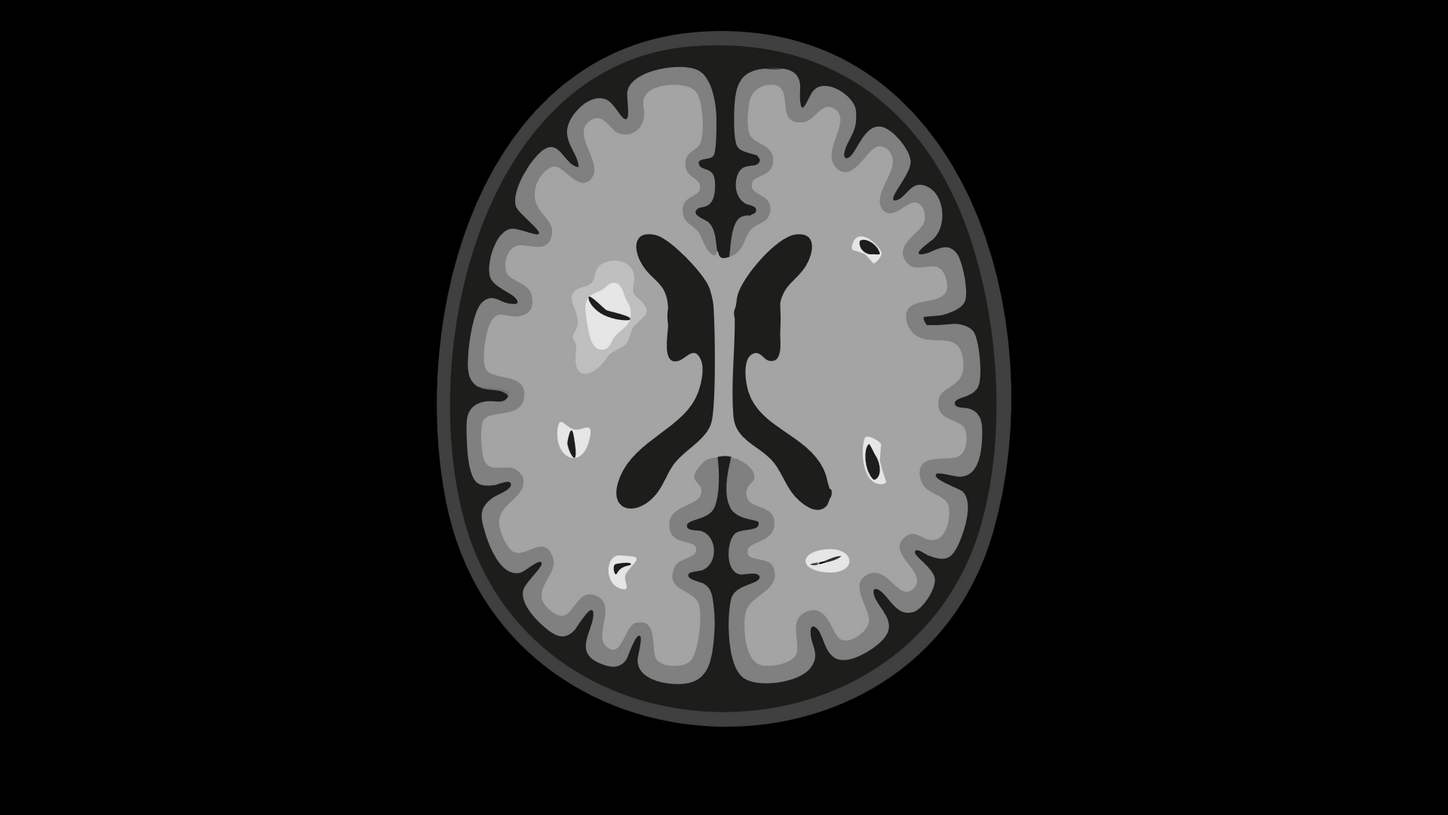
White Matter Hyperintensities (WMH)
As an autoimmune disease, MS is characterized by an overactive immune system, resulting in inflammation areas that lead to the loss of myelin insulation of nerve cells. These active inflammation areas can be seen in MRI on T2-weighted TSE imaging, primarily in the T2 FLAIR contrast. They manifest as hyperintensities, meaning areas with enhanced brightness. As MS patients undergo regular MRI scans to follow-up the disease, these lesions appear at different spatial locations in the brain (dissemination in space, see below). However, as a confounder, such hyperintense areas do not only result from MS, but also from other root causes and sometimes require additional contrasts (e.g., MPRAGE or T2*/SWI) to rule out differential diagnoses.
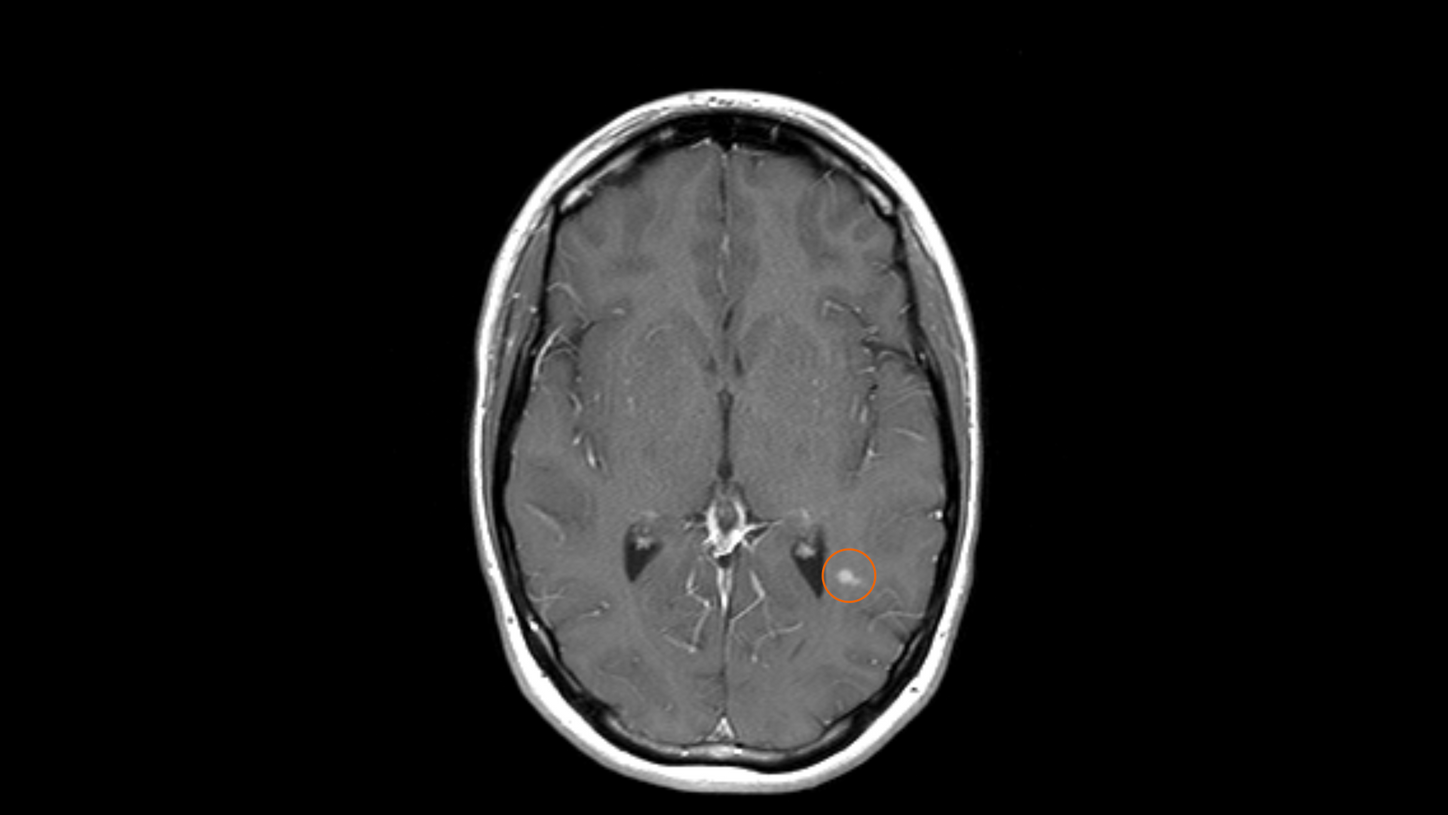
Active lesions
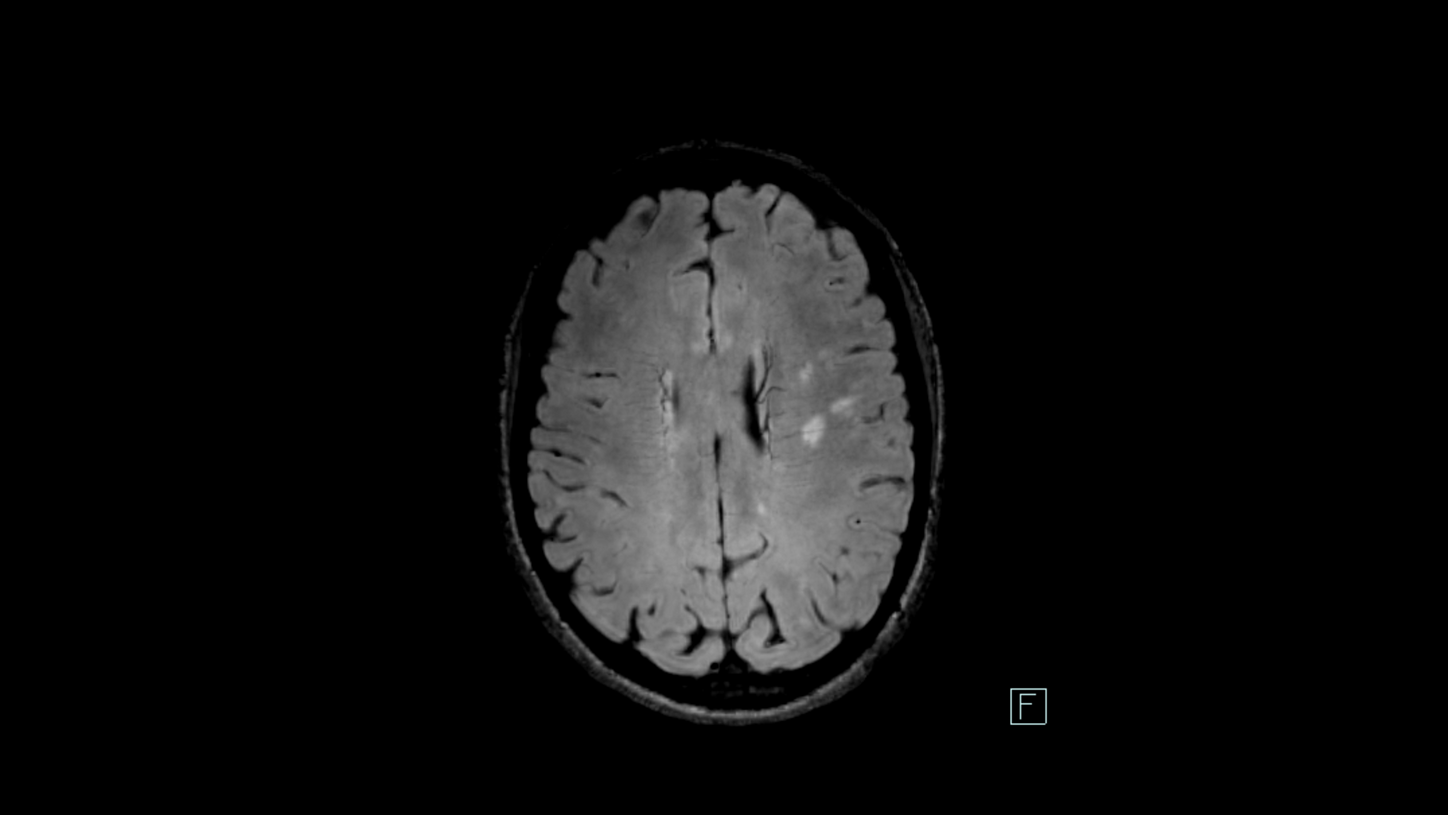
Central Vein Sign (CVS)
T2*-weighted or susceptibility-weighted imaging (SWI) has been shown to be the imaging method of choice to differentiate MS lesions from non-MS lesions. Hyperintensities caused by MS are in the majority of cases focused around a central vein. This vein must be visible in several plane orientations (e.g., axial and coronal) and appears as a dark line or dot, depending on the orientation. It should be central and not along the rims of the WMH. This is the so-called CVS, and it can be visualized by fusing the FLAIR image and the magnitude images of T2* or SWI on MR View&GO or syngo.via.
Paramagnetic Rim Lesions (PRLs)
Diagnosing MS: McDonald criteria
MRI is the method of choice to support diagnosis MS and follow-up its progression over time. Also, it supports therapy follow-up imaging to determine the right treatment for the patient.
The diagnostic guidelines for MS are based on the McDonald criteria – the latest revision is from 20242. Cornerstones for a confident diagnosis are dissemination in space and dissemination in time. What do these terms mean?
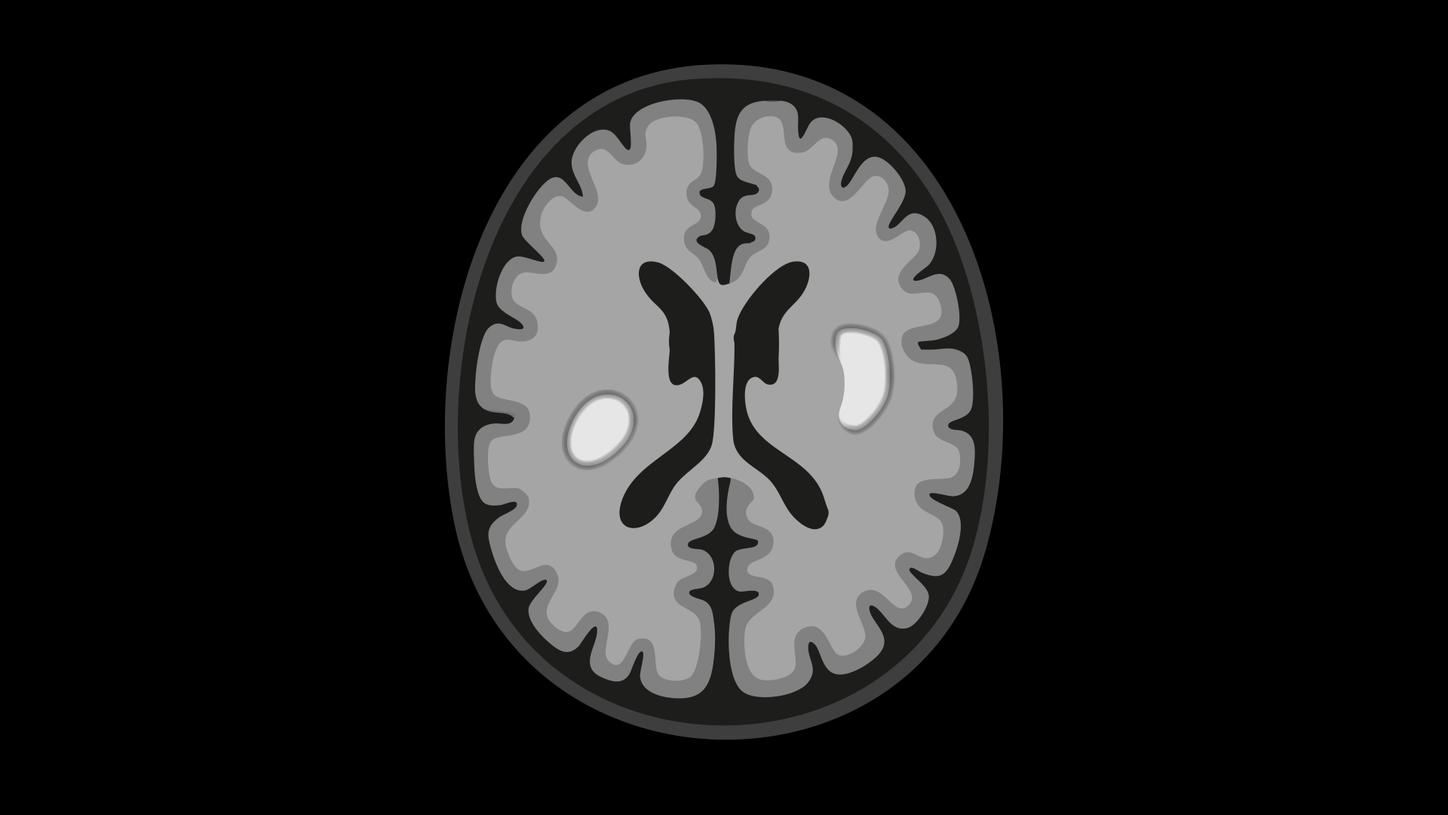
Dissemination in space (DIS)
WMHs in two different brain regions
DIS refers to the development of lesions in distinct anatomical locations within the central nervous system (CNS): intra- or juxtacortical, periventricular, infratentorial, and spinal cord. The 2024 McDonald criteria2 added the optic nerve to these anatomical locations. If MS lesions appear in at least two anatomical locations, DIS has been demonstrated. This acknowledges the multifocal process which is characteristic for MS.
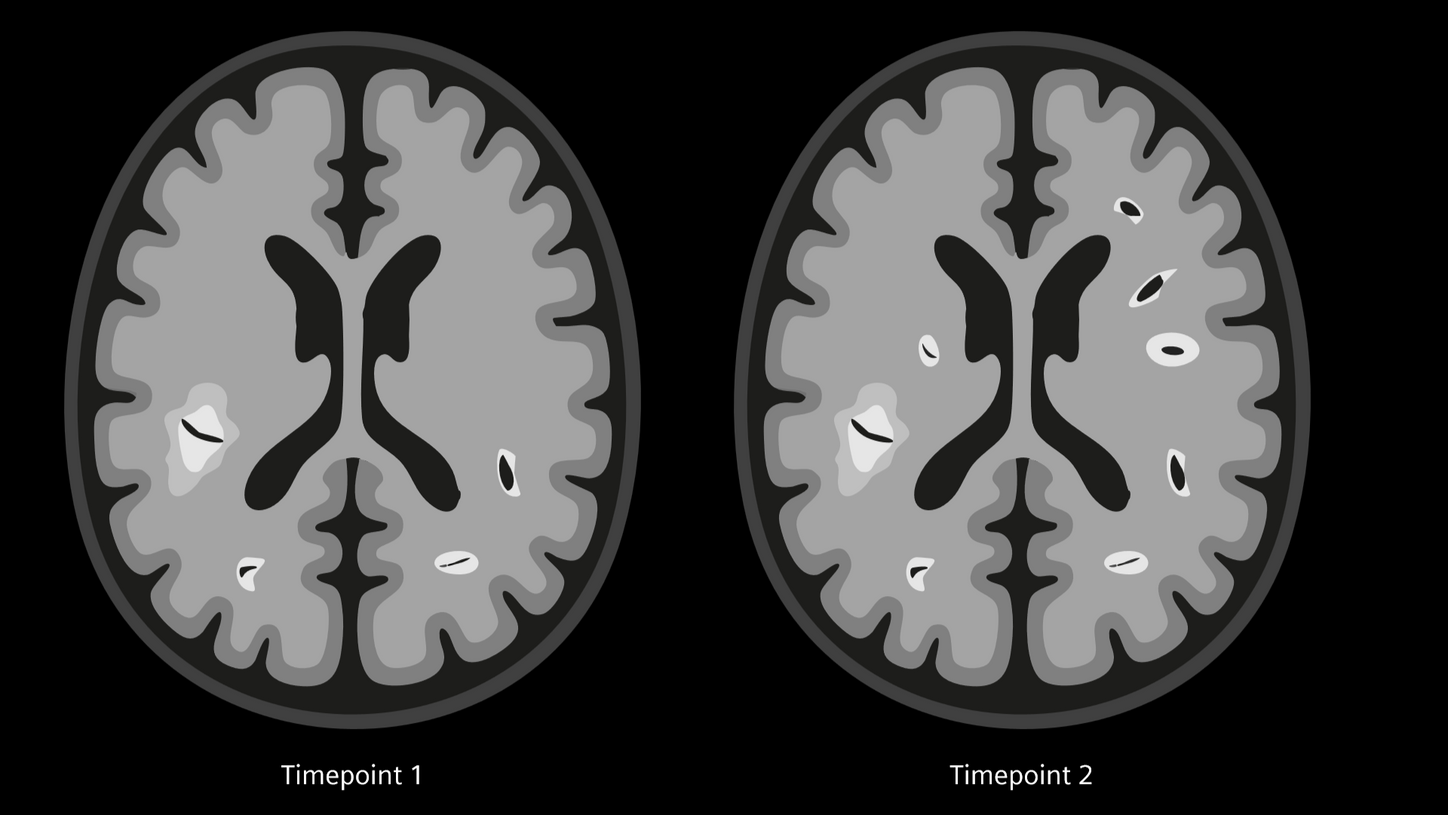
Dissemination in time (DIT)
New lesions at two different points in time
DIT refers to the development of new lesions within the CNS over time, meaning that during different time points of MRI follow-up new lesions can be found which have not been seen before. DIT can be demonstrated via new WMH on T2-weighted imaging as shown above, or new contrast-enhancing lesions in T1-weighted MPRAGE.
Guideline update: 2024 McDonald Criteria
The 2024 update of the McDonald criteria2 emphasized the role of the CVS for a confirmed diagnosis of MS. Instead of demonstrating DIS and DIT, the diagnosis of MS can now be secured by demonstrating either DIS or DIT plus at least six CVS.
Furthermore, PRL can now also support this process: The diagnosis of MS can now be secured by demonstrating DIT plus at least one PRL.
MR protocols for MS diagnostic imaging
Our partners from General University Hospital in Prague, Czech Republic, kindly prepared the required protocols for MAGNETOM scanners.
Our solutions
Clinical Applications relevant for MS
The primary contrasts for MS are T2 TSE, T2 FLAIR, T1 MPRAGE, and T2*-weighted gradient echo imaging. The sequences to obtain these contrasts are available as a standard on all MAGNETOM scanners. In addition to these essentials, we provide other applications that aid at evaluating MS patients.


Community
