
Key points
- This case highlights the usefulness of dual energy CT in suppressing metallic artifacts to detect complications after spinal surgery.
- The accurate diagnosis of the spinal pathology allowed for the selection of appropriate treatment.
History
Diagnosis
Dual energy CT images with iMAR revealed a fracture of the L4 transpedicular screws and posterior pseudoarthrosis at the L3–L4 level, which were not clearly visible in the previous multislice CT due to extensive metallic artifacts (Fig. 1). Additional findings included diffuse bulging of the L3–L4 intervertebral disc, facet joint nonunion, and posterior fixation hardware contributing to moderate spinal canal stenosis (type C according to Schizas [1] – L3–L4 canal compromise) (Fig. 3). A subarticular and left foraminal protrusion of the L5–S1 disc was also observed, partially occupying the left lateral recess and compressing the exiting nerve root (type D – L5–S1 foraminal impingement) (Fig. 2). The patient is currently being prepared for surgery to address screw failure and pseudoarthrosis. Surgical planning also includes decompression of the L5–S1 nerve root.
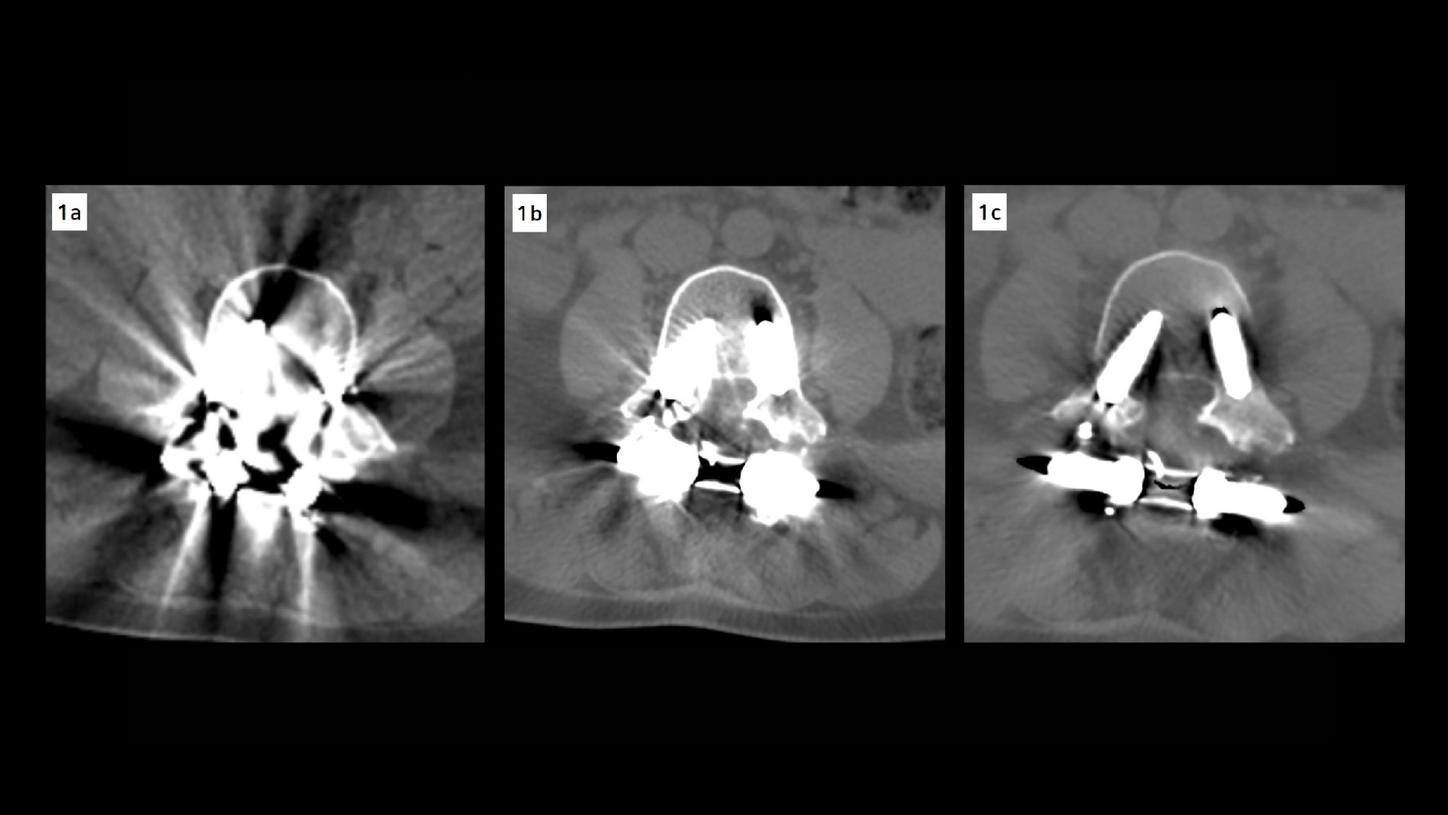
Fig. 1: Axial CT images of the lumbar spine at the L3–L4 discal space. (A) Image acquired on a previous standard multislice CT scanner, shows prominent metal artifacts that obscure the vertebral anatomy and prosthetic components. (B) Image reconstructed using iterative metal artifact reduction (iMAR) at 120 kV, demonstrates improved delineation of bone structures and reduction of streak artifacts. (C) Image reconstructed with iMAR combined with high-energy monoenergetic imaging (140 keV), provides superior image quality with markedly reduced metal artifacts and enhanced visualization of the prosthesis and surrounding anatomy.

Fig. 2: Lumbar spine CT images demonstrating L5–S1 disc pathology. (A) Volume rendering (VRT) reconstruction showing the posterior fixation hardware with evidence of screw fracture at the L4 level. (B, C) Sagittal and axial reconstructions with iterative metal artifact reduction (iMAR) and 140 keV images demonstrate subarticular and left foraminal protrusion of the L5–S1 disc, partially occupying the left lateral recess and compressing the exiting nerve root, consistent with type D L5–S1 foraminal impingement.
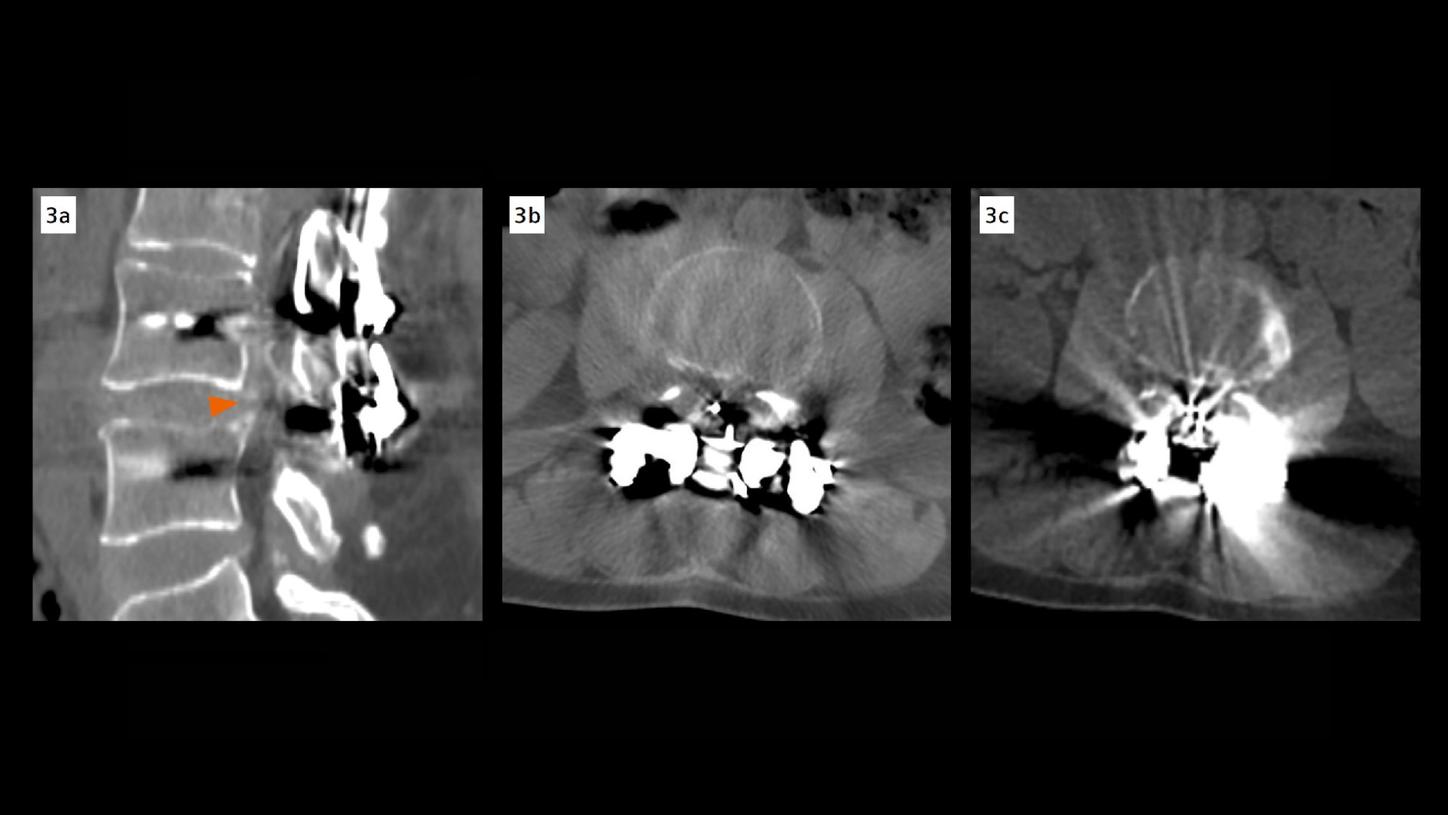
Fig. 3: Axial and sagittal CT images of the lumbar spine at the L3–L4 level. (A, B) Sagittal and axial image reconstructed using iterative metal artifact reduction (iMAR) combined with high-energy monoenergetic imaging (140 keV), show markedly improved visualization of the prosthetic components and surrounding anatomy, revealing moderate spinal canal stenosis. (C) Axial image acquired on a previous standard multislice CT scanner, with prominent metal artifacts that obscure the spinal canal and adjacent structures.
Comments
Postoperative evaluation of the spine in patients with metallic fixation devices presents a diagnostic challenge, as conventional CT imaging is often compromised by extensive artifacts that obscure critical anatomical details. These limitations can hinder therapeutic decision-making, particularly when assessing potential complications such as screw failure, pseudoarthrosis, or neural compression. In this case, dual energy CT imaging with high-energy virtual monoenergetic reconstructions (140 keV), combined with iMAR, enabled a substantial reduction of metallic artifacts. This enabled clear visualization of the L3–L4 segment, which had been inaccessible on earlier standard multislice CT scans. The improved image quality revealed a fracture of the L4 transpedicular screws and posterior pseudoarthrosis at the L3–L4 level – findings that are clinically relevant and indicative of mechanical instability. These alterations, along with diffuse disc bulging and facet joint nonunion, contributed to moderate spinal canal stenosis, correlating with the patient’s symptoms of radiculopathy and functional impairment. Additionally, the scan identified a subarticular and left foraminal disc protrusion at L5–S1, partially occupying the left lateral recess and compromising the exiting nerve root. This finding further supports the need for surgical intervention.
The combined use of dual energy imaging and iterative metal artifact reduction (iMAR) significantly improved image quality by reducing metallic artifacts from the fixation devices. This approach enabled clearer visualization of the spinal canal and foramina, supporting a more accurate assessment of postoperative complications and providing crucial information for surgical planning.
Examination Protocol