
More than 40 years ago, Siemens set out on a journey that has taken CT from morphological diagnosis to functional imaging. It is 10 years since radiology was revolutionized by the exciting concept of Dual Source CT. This was a technology with fantastic potential, both for users of DSCT and for Siemens.
The history of CT technology at Siemens began in 1974. With Siemens’ CT scanner SIRETOM, it became possible for the first time to perform cranial scans in a scan time of seven minutes.
During the 1980’s, CT became part of clinical routine. Using fan-beam detectors, a complete cross section of the patient’s body could be captured in a single run, while the acquisition time per image was reduced to a few seconds.
A key development was the introduction of spiral CT in 1989. With a rotation time of one second, whole organs could now be examined within one breath-hold of the patient.
At the end of the century, multislice CT opened up the way for new clinical applications: CT angiography and cardio CT.
Spurred on by competition: In the 1990’s, the team of researchers and developers at Siemens faced a particular challenge, the electron beam CT scanner produced by the U.S. firm Imatron. While mainly experimental, the electron beam scanner was the first device to achieve an exposure time of 50 ms per image, making cardiac CT possible. However, while temporal resolution was good, spatial and contrast resolution were restricted, limiting the amount of information that could be derived from a heart scan. A further weakness was that the heart was the only organ for which images at acceptable quality could be produced.
A (r)evolutionary concept in cardiac CT with 64-slice
Using multislice technology, Siemens pioneered the development of cardiac imaging with conventional CT. In 1999, the 4-slice CT scanner SOMATOM Volume Zoom was the first mechanical CT scanner capable of imaging the heart and the coronary arteries with diagnostic image quality. The introduction of 64-slice CT in 2003 meant that examination times could be reduced. The use of thin slices in clinical routine allowed for improved spatial resolution, and interactive three-dimensional image displays replaced analysis of individual slices. With a rotation time of 0.33 s and temporal resolution of 165 ms per image (a half-rotation was needed to capture enough data for one image), cardiac imaging was routinely feasible at low to moderate heart rates, and a whole heart could be scanned in five seconds.

With 64-slice CT, cardiac CT scans with reliably good quality were only possible for patients with heart rates below 70 beats per minute. Therefore, drugs were frequently used to lower the heart rate but that is not an option for some patients. Although the potential of cardiac CT was recognized, the limitations of 64-slice imaging prevented it from becoming part of clinical routine in cardiology.
In 2002, the Siemens research team began discussing with clinical specialists how cardio CT could be improved, given that the temporal resolution of single source CT could not be increased beyond a certain point. It was recognized that no device based on this principle would be able to match the temporal resolution range of 50 ms achievable using electron beam CT.
A breakthrough with Dual Source CT

Despite its lower temporal resolution, the conventional third-generation CT scanner had a higher spatial resolution than the electron beam scanner and was better at showing slight differences in contrast, meaning that overall image quality was significantly better. Taking this as their starting point, in 2002 the development team came up with an ambitious idea. In place of the single source principle, they argued that faster imaging could be achieved by installing two detector systems in one gantry, at an angle of 90° to each other. The foundations for the development of dual source technology had been laid.
This innovative idea was not embraced by everyone. Some critics would have rather followed the traditional way of simply increasing the detector width. In addition, there were many physical obstacles, such as the limited space on the gantry, the complex system control, or cross-scattered radiation. However, the highly motivated team at Siemens were convinced that the dual source principle could be implemented in practice. The more doubts and objections they encountered, the more determined they became to overcome this challenge.
Professor Thomas Flohr, PhD, a member of the dual source research team, reports: “We had recognized the opportunities presented by cardio CT and were also convinced that a Dual Source CT system would have applications beyond cardiology. There was something of a gold-rush mood in the team. We were electrified by the idea.” Intensive collaboration with medical advisory boards then effectively led to the development of the first dual source scanner that could be used in practice, with new, compact tube technology and high performance (the rotating envelope Straton tube).
"We were highly confident that dual source would offer possibilities beyond cardiology."

In 2005, following a three-year development phase, Siemens launched the first Dual Source CT scanner, the SOMATOM Definition.[1,2] Its introduction caused a sensation in the field. SOMATOM Definition could achieve a temporal resolution of 83 ms per image, and a quarter-rotation was sufficient to allow each of the two detector systems to capture enough data to produce an image. For the first time, the heart could now be imaged without motion artifacts at high heart rates or in cases of arrhythmia.[3]
The introduction of Dual Source CT was critical in enabling cardio CT to become part of clinical routine over the next few years. It has also played a major role in shaping the potential applications of CT in the field of cardiac imaging.[4]
Expanding the application for Dual Source CT
From the start, Dual Source CT was intended to have application not just in cardiology but also in other specialties such as oncology and pediatrics. To achieve this, the principle of scanning at different voltages was integrated: dual energy CT.
Dual energy CT reveals not only the morphology, but also the chemical composition of the scanned organs. This new technology aims at developing CT into a tool for functional as opposed to purely morphological imaging.[5] Physicians can use it to evaluate the local iodine uptake in contrast-enhanced scans and to compute virtual non-enhanced images, to automatically remove the bones from CT angiographic studies. Another example is the characterization of tissue or differentiation of deposits such as kidney stones. The absorption of iodinated contrast medium by a tumor can also serve as an indicator of local perfusion and thus as a marker of tumor dignity.
The introduction of the SOMATOM Definition Flash in 2009 led to further optimization. This had its origins in a suggestion by Professor Jacques Remy from Lille, who was particularly enthusiastic about the high scan speeds that could be achieved by utilizing both measurement systems of a Dual Source CT. In a discussion with Thomas Flohr, the idea to use a very fast spiral scan to image an entire heart during one heartbeat was born. This became the basis for the Flash scan mode. Thanks to its high scan speed of 458 mm/s, a heart could be scanned in only 0.22 seconds, meaning that at low heart rates a CT scan could be carried out in a single heartbeat. In terms of radiation dose, Flash mode is the most efficient method of cardiac imaging, as it captures only the minimum amount of data needed for image reconstruction. This means that a heart can be imaged with a radiation dose of only 1 mSv, one tenth of that required by other systems.
Today, SOMATOM Definition Flash is the gold standard in cardio CT, with excellent image quality and at low radiation dose. The entire heart can be imaged with a temporal resolution of 75 ms. In addition, flexible scan modes allow clinicians to obtain morphological findings, examine coronary arteries, plan TAVI procedures, and capture data for assessing myocardial perfusion. Even heart-scanning without beta-blockers may become possible.

Fig. 3:
Cardiac imaging – in Turbo Flash mode, scanning can be sped up to 737 mm/s. With CARE kV and CARE Dose4D, exposure dose can be individualized automatically. This case was acquired in 0.12 s at 80 kV, 0.28 mSv, using 30 mL contrast agent only. Coronary diseases can be excluded confidently as shown in VRT and curved MPR images in great detail.
Young patients are a challenge, as generally they need intensive preparation, sedation, and subsequent monitoring when undergoing a CT scan. As the Flash mode combines a scan speed of 458 mm/s with a temporal resolution of 75 ms, the average time for a pediatric scan is less than a second, allowing physicians to reevalute the need for sedation.
Dual source dual energy CT (DSDE) is improved with the SOMATOM Definition Flash because of the increased coverage offered by its second detector (33 cm). A tin filter can be used to optimize spectral separation, which significantly reduces the radiation dose necessary for dual energy imaging and allows for “doseneutral” dual energy scans. Dual energy CT has many potential applications in oncology. It meets all the diagnostic requirements for detection and visualization. That enables physicians to evaluate the iodine uptake of tissue lesions in one scan, with radiation doses similar to those for a conventional 120 kV scan.
State-of-the-art in morphological and functional imaging
Siemens has worked consistently to enhance the temporal and spatial resolution of its DSCT. The result is the SOMATOM Force. Using the newly developed Vectron X-ray tube, good image resolution and high image quality can be maintained even at very high tube currents and low tube voltages.
Vectron X-ray tubes have a power capacity of 120 kW, while the tube voltage can be set at between 70 and 150 kilovolts (kV). In many examinations, especially those involving contrast media, using low voltages can be beneficial, as it makes for a better contrast-to-noise ratio. Due to technical limitations, 70 kV or 80 kV CT used to be reserved exclusively for children and slim patients. With the Vectron tubes and its enormous power reserves at low kV (up to 2x 1300 mA), adults and even patients with a high body weight can be examined in a short time window and at low tube voltages. This means that contrast can be maintained while reducing radiation dose.
Alternatively, the high contrast-to-noise ratio at low tube voltages may be used in a different way: Early clinical experience based on imaging of the left ventricle and aortic root (TAVI studies) demonstrated that a reduction of contrast media administration may be possible using SOMATOM Force’s Turbo Flash Mode and its low kV/high mA capabilities.
A study on coronary CT angiography was recently published: The authors report that using SOMATOM Force at 70 kV results in a lower radiation exposure (0.44 mSv at 70 kVp instead of 0.92 mSv at 100 kVp) as well as less contrast medium volume (45 mL instead of 80 mL) compared to a state-of-the-art CT scanner employing 80 kV or 100 kV tube voltage settings. Concurrently, image quality could be maintained. The study is based on the examination of 45 patients. Image quality was measured using image-based objective criteria, such as contrast-to-noise ratio and image noise, and by the subjective assessment of two radiologists.[6] This is particularly beneficial for older and chronically ill patients with impaired renal function, whose kidneys have low tolerance for iodinated contrast media.
In Turbo Flash mode, the scan speed is increased to 758 mm/s. This, together with a reduction in radiation dose, makes this CT scanner the ideal diagnostic tool for examining small children, even if they will not lie still.
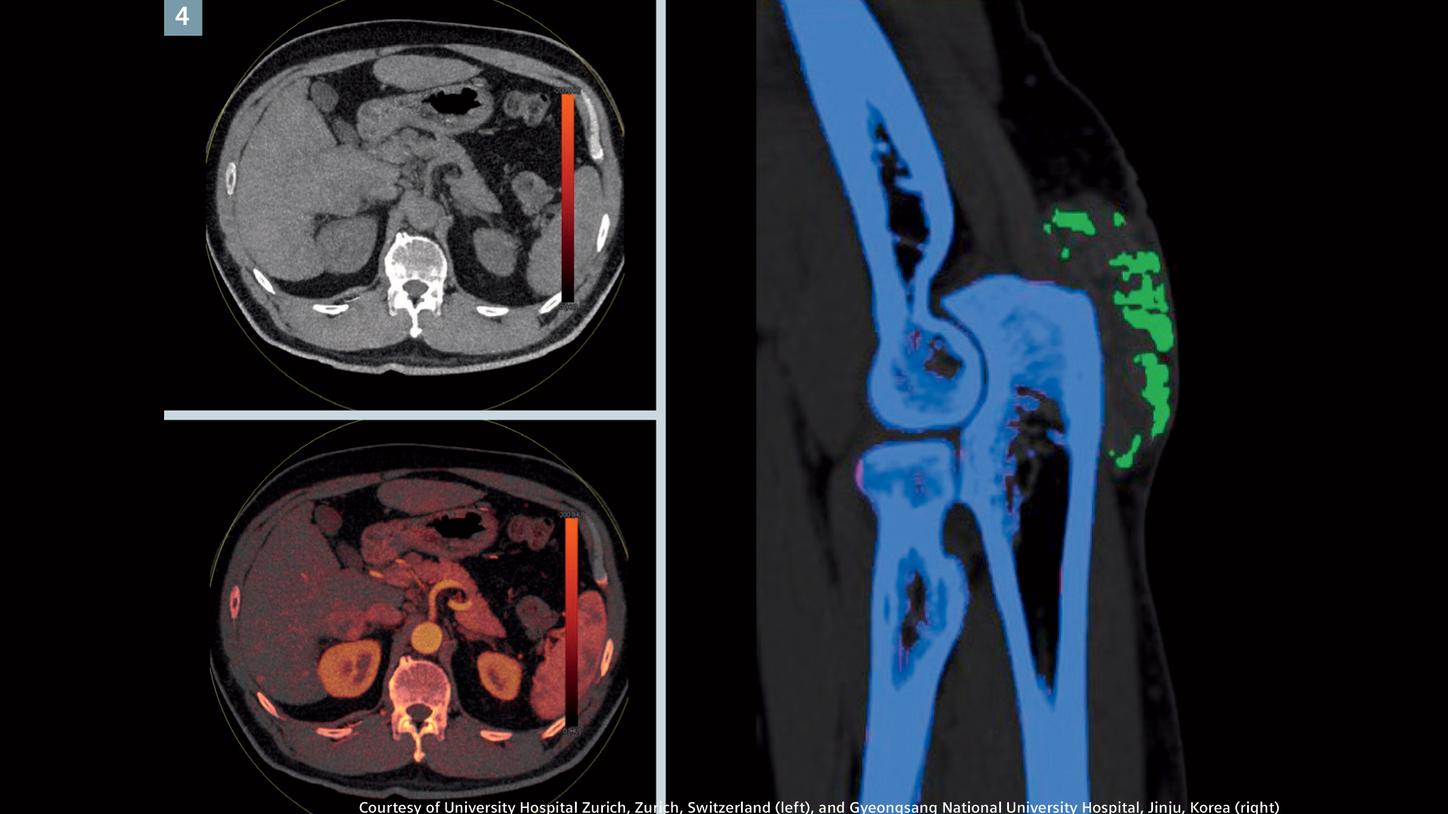
Fig. 4:
Dual energy imaging – the Selective Photon Shield allows dedicated filtration and better separation of the low and high energy spectrum, which significantly improves material differentiation in dual energy imaging. A virtual non-contrast (VNC) and a fused VNC/iodine image (left) reveal an enhanced lesion in the right hepatic lobe, segment VI, indicating a metastasis. Gout crystals are demonstrated in the posterior elbow (right).
As SOMATOM Force incorporates dual energy technology, physicians are able to differentiate tissue and materials chemically even where they have the same density value. This functional imaging opens up the path to new approaches to cancer diagnosis. Based on information of this imaging, the physician, for example, can characterize tumors and assess how a patient responds to treatment. Moving beyond dual energy data capture, the use of temporally resolved perfusion measurements – already well-established in stroke diagnosis – is now finding its way into oncology.
With its excellent temporal resolution, SOMATOM Force is able to minimize movement artifacts, meaning that it can be used with patients who are unable to hold their breath due to illness, age, asthma or shortness of breath, or trauma.
Future potential of Dual Source CT
Dual Source CT technology has opened up some promising avenues for research institutions. SOMATOM Force has set the benchmark for mechanical features such as temporal resolution, scan speed, and low radiation dose, but there are many applications that continue to be developed.
Some of these relate to scan specificity, for example. A 60-percent stenosis of the coronary arteries can be accurately diagnosed using SOMATOM Force. However, at the moment further examinations are needed to clarify whether a stenosis is affecting the blood supply to the heart muscle. In the future, it may be possible to determine this using Dual Source CT alone, rendering further examinations with a heart catheter, MR, or SPECT unnecessary.
SOMATOM Force allows the lungs to be imaged at extremely low radiation doses. The Selective Photon Shield optimizes the X-ray spectrum in high-contrast applications without iodinated contrast medium, such as pulmonary imaging. This may potentially play a supportive role in screening for lung cancer.

Fig. 5:
Pneumonia – the Selective Photon Shield II optimizes the X-ray spectrum, which significantly improve the air/soft tissue contrast. MPR images demonstrate bilateral areas of consolidation and ground-glass attenuation with superimposed interlobular septal thickening. CT scan was performed without breath-hold in Turbo Flash mode, with an effective dose of only 0.04 mSv, which is less than a standard X-ray radiography examination.
In the field of abdominal and pelvic medicine, the ability of Dual Source CT to capture the function as well as the morphology of the tissue to be examined opens up the possibility of using local tissue perfusion as a marker in treatment monitoring – for example, in the diagnosis and treatment of hepatic and gastrointestinal tumors and in the detection of bone metastases.
With the help of biochemical markers, it will be possible to offer tomorrow’s patients diagnosis and treatment tailored to their individual needs. SOMATOM Force provides strong hopes that we will be able to provide the diagnostic data needed for early detection, precise characterization, and removal of tumors and metastases.
Professor Thomas Flohr: “This isn’t the end of the story. We remain committed to exploring the whole range of possible applications for Dual Source CT.”
Another focus for the future is workflow automation. Overall, users require better and simpler integration of CT into clinical routine. There is, therefore, scope for optimizing the quality standards of clinics and practices in relation to diagnosis and treatment. Patients also benefit from workflow automation in terms of waiting times, treatment processes, and outcomes. Not least, improved automation of workflows could give impetus to clinical research projects and the development of new approaches to diagnosis and treatment.
Related links
About the Author
Ruth Wissler, MD studied veterinary and human medicine. She is an expert in science communications and medical writing.