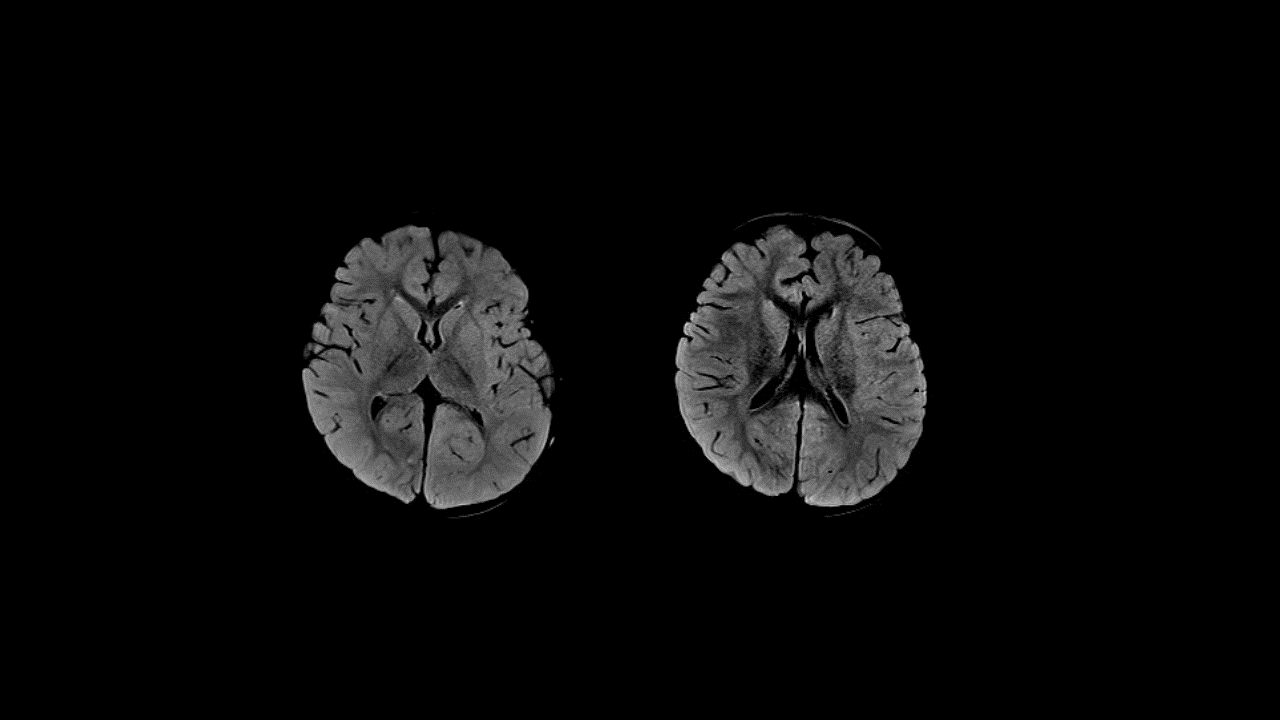

Diffusion B1000
Diffusion-weighted imaging is a core sequence in routine clinical imaging of children with acute leukoencephalopathy.
In the last decade, many atypical causes of acute encephalopathy have emerged in the pediatric population. One such condition is acute encephalopathy with Restricted Diffusion (ALERD), in which routine MRI sequences can appear normal.
Below, we have reviewed this condition›s etiology, types, and clinico-radiological features.
Conventionally, diffusion-weighted imaging is acquired using a single-shot diffusion-weighted echo planar imaging (EPI) sequence. However, this sequence suffers from a lower spatial resolution and susceptibility-based geometric distortions. RESOLVE diffusion is a segmented readout EPI acquisition with excellent spatial resolution, nearly no susceptibility, and geometrical distortions.
Equipment
Imaging is performed on the Siemens Healthineers MAGNETOM Vida 3T system, equipped with BioMatrix Technology. Protocols are optimized for image quality and acquisition time. The industry-unique 20-channel BioMatrix™ Head/Neck coil with CoilShim and SliceAdjust is used for neuroimaging. This technology allows the acquisition of patient-independent, consistent image quality.
MR Techniques
We performed ultrafast emergency GoBrain protocols with a high-resolution RESOLVE diffusion.
Imaging:
Protocols includes:
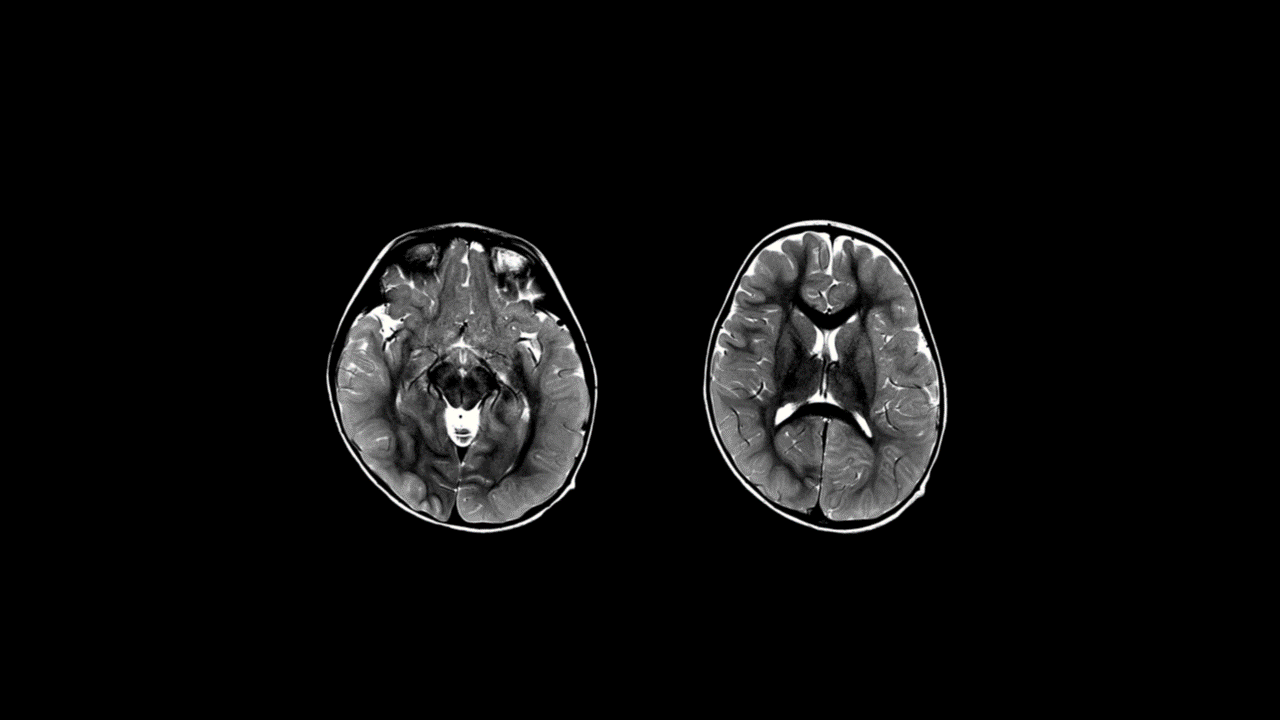
- T2 TSE Axials
- T2 TSE Darkfluid
- T1 TSE Axials
- Gradient echo T2*
- Diffusion
Clinical Presentation
2-year-old female with seizure and fever for 1–2 days followed by spontaneous improvement and then readmitted with fever for 1 day with symptoms of drowsiness and recurrence of seizures (multiple episodes in 24hrs).
On Examination
Child drowsy, moving all 4 limbs, pupils equal with no meningeal signs.
Imaging Findings
Symmetric areas of Restricted Diffusion in the bilateral temporal and parieto-occipital subcortical and periventricular white matter and in the bilateral frontal subcortical white matter. The white matter depicts a “bright tree appearance” which represents high-signal intensity on DWI B1000 in the subcortical white matter, akin to tree branches.
Areas of Restricted Diffusion are also seen in the leftthalamus, caudate nuclei bilaterally, dorsal pons, inferior cerebellar cortex in the paramedian location and in the superior vermis.
Subtle thickening of the cortex in the bilateral parieto-occipital regions with mild blurring of gray-white matter interface in these regions.
No abnormal leptomeningeal or brain parenchymal enhancement.
There is no evidence of hydrocephalus.
Imaging features suggest diffuse type Acute Leukoencephalopathy with Restricted Diffusion - ALERD
Clinical Features, Etiology and Pathogenesis
ALERD is a clinico- radiological syndrome - a viral-associated encephalopathy seen in childhood described mainly from the Asian continent.
Clinical presentation is with prolonged seizure with fever for 1–2 days followed by spontaneous improvement, followed by worsening of clinical state with cluster of seizures, altered sensorium 3–4 days later. The second phase is characterized by areas of Restricted Diffusion on MRI.
MRI reveals restricted areas of diffusion seen in both gray and white matter - a hallmark of this condition.
It has been reported mainly from East Asia. In a series of 44 patients from Nagoya University, Japan, causative pathogens isolated were human herpesvirus-6, adenovirus, rotavirus, influenza virus, Mycoplasma pneumoniae, Enterovirus type Coxsackievirus A6, Escherichia coli O157:H7, and Streptococcus pneumonia.
Most patients show hypercytokinemia in the form of elevated interleukin-6 (IL-6), IL-8, and IL-10 and tumor necrosis factor in the serum and IL-4, IL-6, and IL-8 in the cerebrospinal fluid (CSF). Excitotoxic injury with delayed neuronal death is hypothesized as a possible mechanism.
In ALERD, no autoantibodies have been found.
The pathophysiological mechanism of ALERD does not require direct infection of the central nervous system.
Laboratory Abnormalities
In diffuse ALERD, increased liver enzymes, hyperglycemia, hyperCKemia, and metabolic acidosis are noted.
In central-sparing, ALERD laboratory abnormalities are mild.
The CSF examination is usually normal. This finding helps in ruling out the infectious causes of acute febrile encephalopathy.
Two types of ALERD were identified based on the distribution of brain lesions:
1 Diffuse type
There are diffuse areas of Restricted Diffusion. This type is associated with rapid and severe deterioration of consciousness.
Seizures at the onset of the disease are not always present. It has a poor outcome and can be associated with mortality. Known sequelae are cognitive impairment, epilepsy, and behavioral problems.
A systemic inflammatory response in which multiple organ failure, shock and disseminated intravascular coagulation are often observed.
2 Central sparing type
There is sparing of the central regions of the brain. It is a relatively mild phenotype. A biphasic clinical course is a characteristic of this group. Onset is with prolonged seizure with fever followed by improved consciousness.
Clustered seizures, signs of frontal lobe dysfunction, and worsening of consciousness become apparent at 3–4 days after onset.
Coma is uncommon and various degrees of cognitive impairment are observed as neurologic sequelae.
Outcome
In diffuse ALERD, up to 5%–10% mortality has been reported, while in the central-sparing ALERD/AESD, there have been no reports of death. More than 2/3rd of children with ALERD develop sequelae. Postencephalopathic epilepsy is seen in 1/4th of children.[4]
Other long-term sequelae include hyperactivity with language delay, cognitive impairment, spasticity, dyskinesias, and hemiparesis.
Conclusion
ALERD is a rare cause of acute encephalopathy. Diagnosis is based on identifying restricted diffusion in the white matter and/or cortex on DWI in the MRI of the brain.
MRI may appear normal in the first 3–4 days, hence repeating the MRI scan after 5 days if ALERD is strongly recommended.
Routine imaging sequences like Spin Echo, Turbo Spin Echo, Inversion Recovery, and Gradient Echo may appear normal in
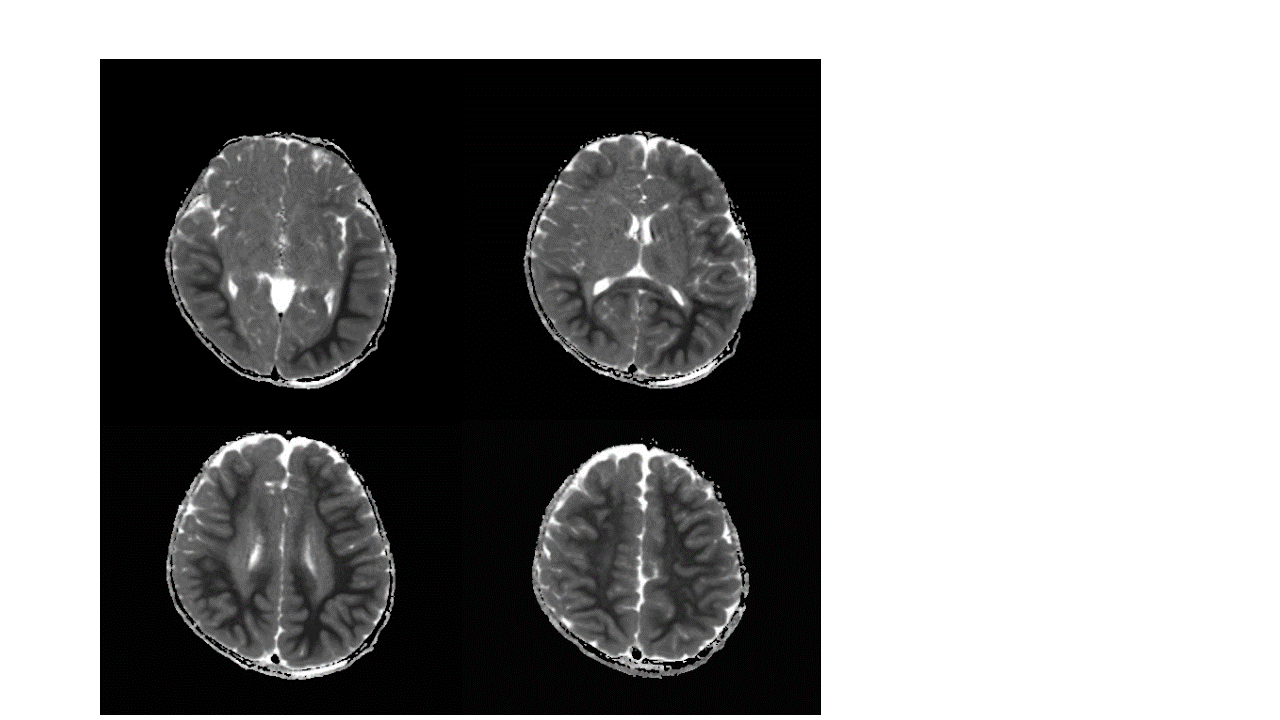
ALERD, and significant findings can be missed. On the other hand, Readout Segmented EPI sequences (RESOLVE) and its ADC maps have the unique ability to highlight the presence of restricted diffusion and, therefore, aid diagnosis.
Contact

HOD and Specialist, Radiologist
NMC Royal Hospital Sharjah, UAE