
Case Presentation and Investigation
Material and Methods
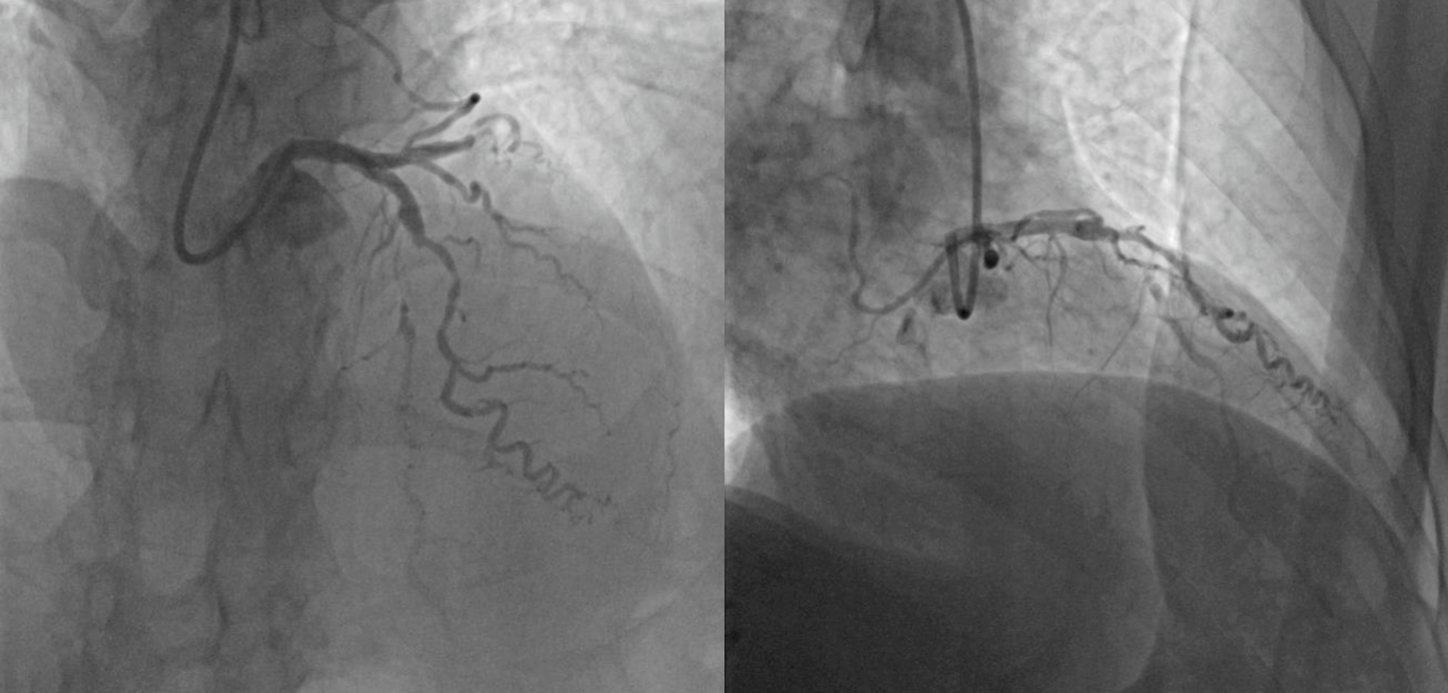
Review of coronary angiography revealed total occlusion of the left anterior descending (LAD) artery at its mid-segment, with retrograde filling from epicardial collaterals originating from the diagonal branches. The length of the occlusion was approximately 20 mm, with no significant calcification or tortuosity. The distal vessel was of good caliber, making it amenable to potential revascularization.
A 50-year-old male patient, previously treated for hypertension for several years, presented with complaints of angina pectoris (class II) and dyspnea (class II) for a duration of 6 months. His echocardiography showed severely impaired left ventricular systolic function, with an ejection fraction (EF) of 25-30%, indicating significant cardiac dysfunction. Multi-slice computed tomography (MSCT) coronary angiography was requested and revealed significant coronary artery disease involving the LAD and other vessels, specifically the left circumflex artery.
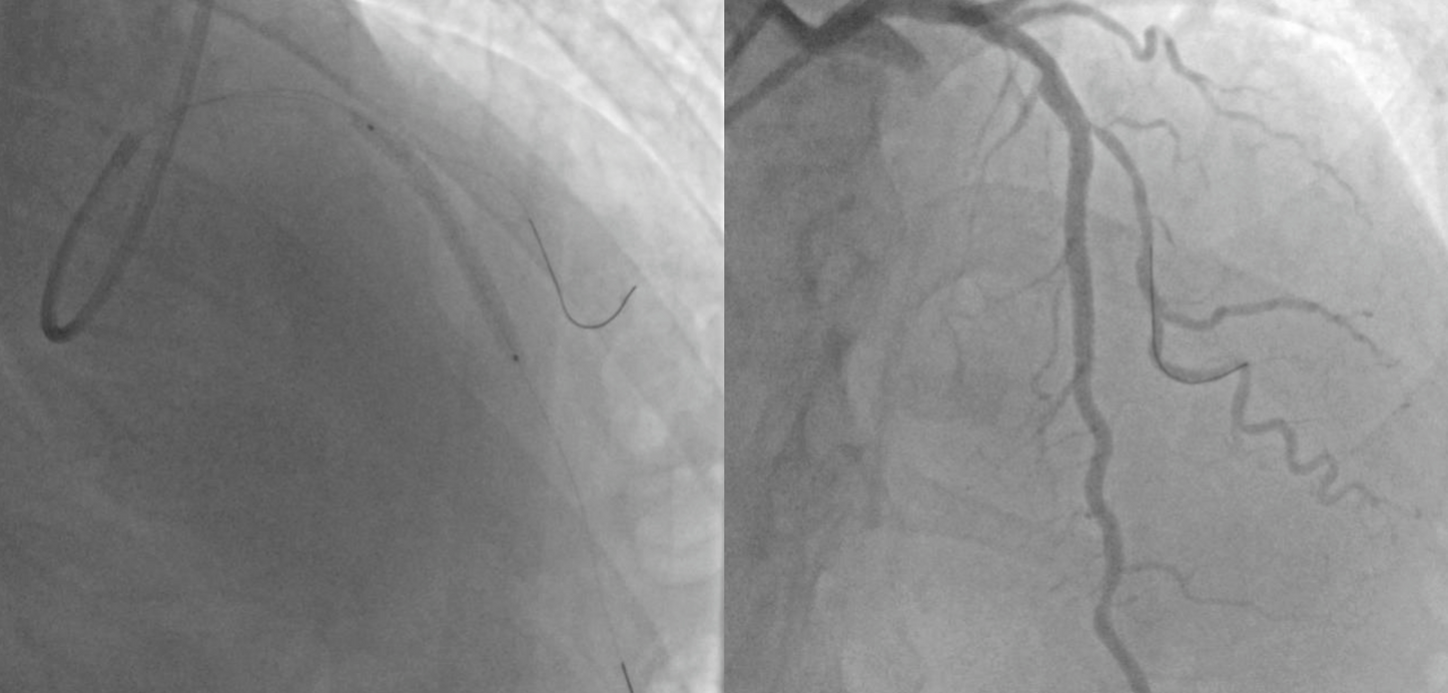
Coronary angiography confirmed chronic total occlusion (CTO) of both the LAD and left circumflex arteries. Viability assessment using cardiac MRI confirmed a transmural scar in the left circumflex artery territory, with a viable LAD artery territory. This finding indicated that revascularization of the LAD artery could potentially improve the patient’s symptoms and quality of life. Following a heart team discussion, revascularization of the LAD artery via CTO-PCI was planned, given the favorable distal vessel caliber and the high likelihood of symptomatic relief, which could have a significant impact on the patient’s functional status and overall prognosis.
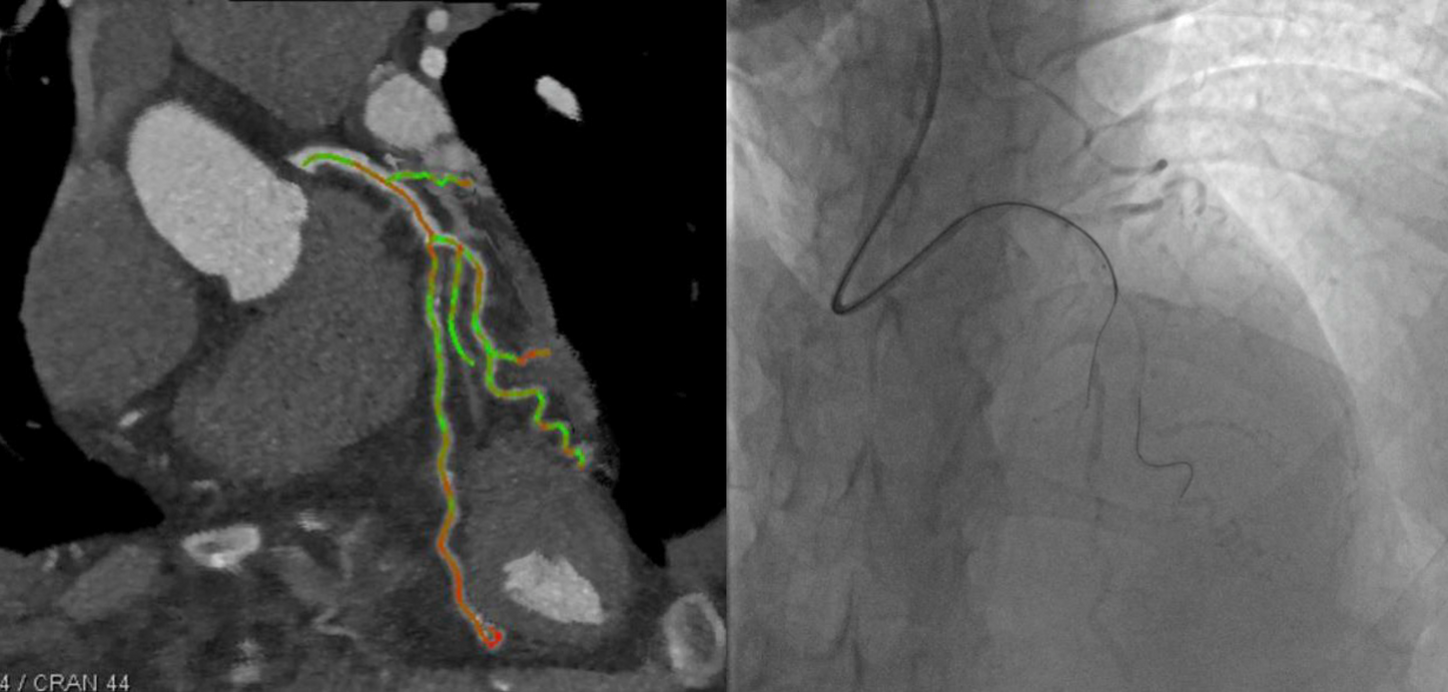
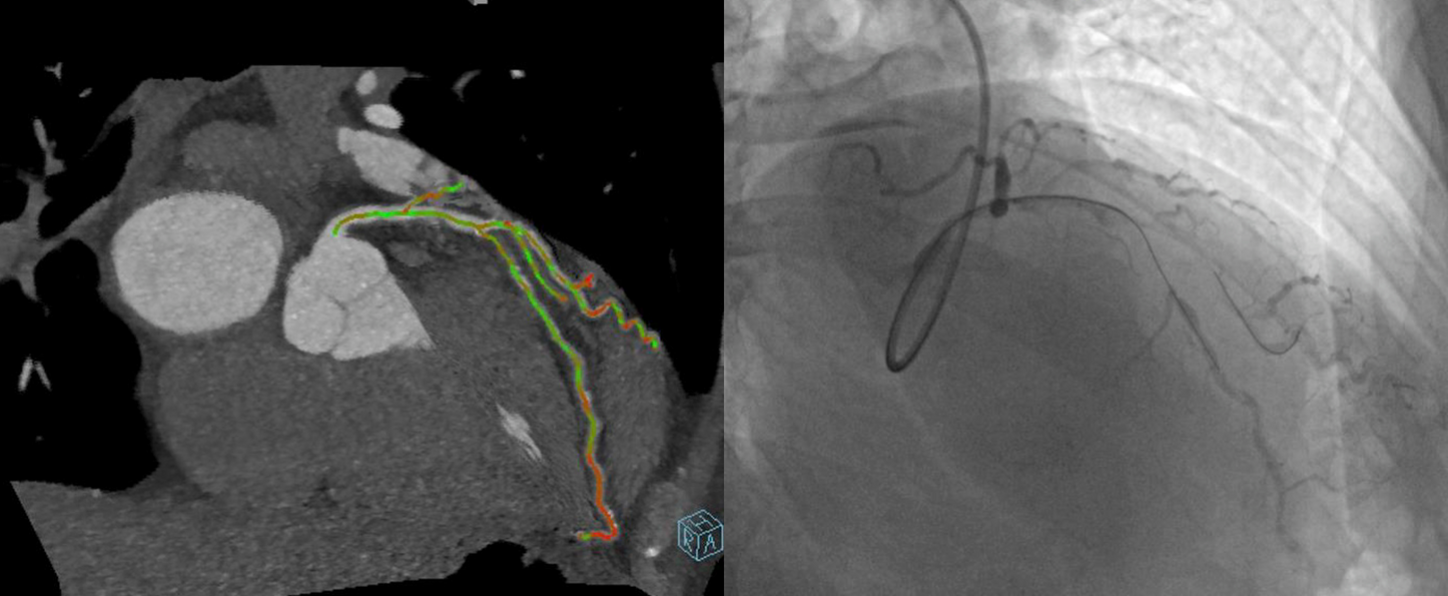
"The integration of syngo CTO Guidance in interventional procedures for CTO offers significant advantages. This technology facilitates wire crossing and positioning by providing side-by-side guidance with fluoroscopy and CTA images. It also offers valuable insights into calcification, as well as the true length and course of the occluded vessel segments, aiding in wire selection, procedural orientation, and overall procedural success."
