Introduction
When imaging the heart, arrhythmia (any disturbance of the normal rhythmic beating of the heart or myocardial contraction) might be a nightmare for the acquisition of clinically optimal images. Over the past years, the resultant motion artifacts in those patients with arrhythmia produced sub-optimal imaging. Nevertheless, given the recent advancements in CT technologies, these challenges could be overcome using advanced CT scanner technical capabilities such as Native Temporal Resolution. Temporal resolution - the time required to capture every single image, can be considered as the speed of a camera taking a snapshot from a moving object. The ‘native spatial resolution’ which can be achieved by the scanner without using special modes such as multi-segment reconstruction or motion correction software techniques play a major role in imaging such patient groups.
New technologies that affect cardiac CT imaging practice in arrhythmic patients
Native Temporal Resolution
Sub-second Scanning - Rotation Speed
In CT imaging, the high image acquisition speed leads to decreased motion artifact and reduced radiation exposure. One of the key features of the scanners is the fast gantry rotation, implying better temporal resolution to reduce motion artifact and patient’s radiation dose. High temporal resolution and selection of the least moving phase of the cardiac cycle for image reconstruction are essential for obtaining coronary CT angiographic images that are free from cardiac motion artefacts with our SOMATOM Force CT Scanner with sub-second rotation time of 250 mSec, one may achieve in plane temporal resolution of up to 66 ms (and down to 33 mSec using 2-segment reconstruction), which can be regarded as one independent of the heart rate.
All patients were scanned on a SOMATOM Force Dual Source CT scanner with the adaptive prospective CorAdSeq mode. Prospective ECG-triggered sequence (CorAdSeq) protocol in the DSCT helps to obtain high quality images and leads to a desirable diagnostic performance. Furthermore, it results in a reduced radiation dose. Adaptive sequence axial mode will omit or repeat scan when ectopic beat is detected, further editing the ECG Phase reconstruction, using either relative (%) or absolute (mSec) time parameters of R-R interval on concurrently obtained ECG data. Automatic exposure control system-based tube current modulation (CARE Dose4D, Care kV and flex padding, and ADMIRE) are applied to further reduce the patient’s radiation dose. CARE Dose4D automatically adjusts the mA and CARE kV automatically selects the optimal kV for the patient’s body size. The aim of applying CARE kV is to optimize contrast-to-noise ratio (CNR) and dose.
Artificial Intelligence in Cardiac Imaging
Artificial Intelligence (AI) - based arrythmia correction – FAST Cardio Algorithms (Fully assisted scanner technologies) continually monitor the patient’s heartbeat and suggest the right protocol according to the heart rate. During the scan, the arrhythmia detection and scan rejection algorithms can hold the scan upon encountering an arrhythmia and restart the scan when the arrhythmia ends, allowing the precise capture of the desired cardiac cycle phase. FAST Planning adapts the scan range to your patient’s anatomy automatically, reducing over scanning and increasing consistency. FAST 3D Align: adapts the reconstruction range to your patient’s anatomy without any manual interference.
Study discussion – Clinical proof 1

Case presentation
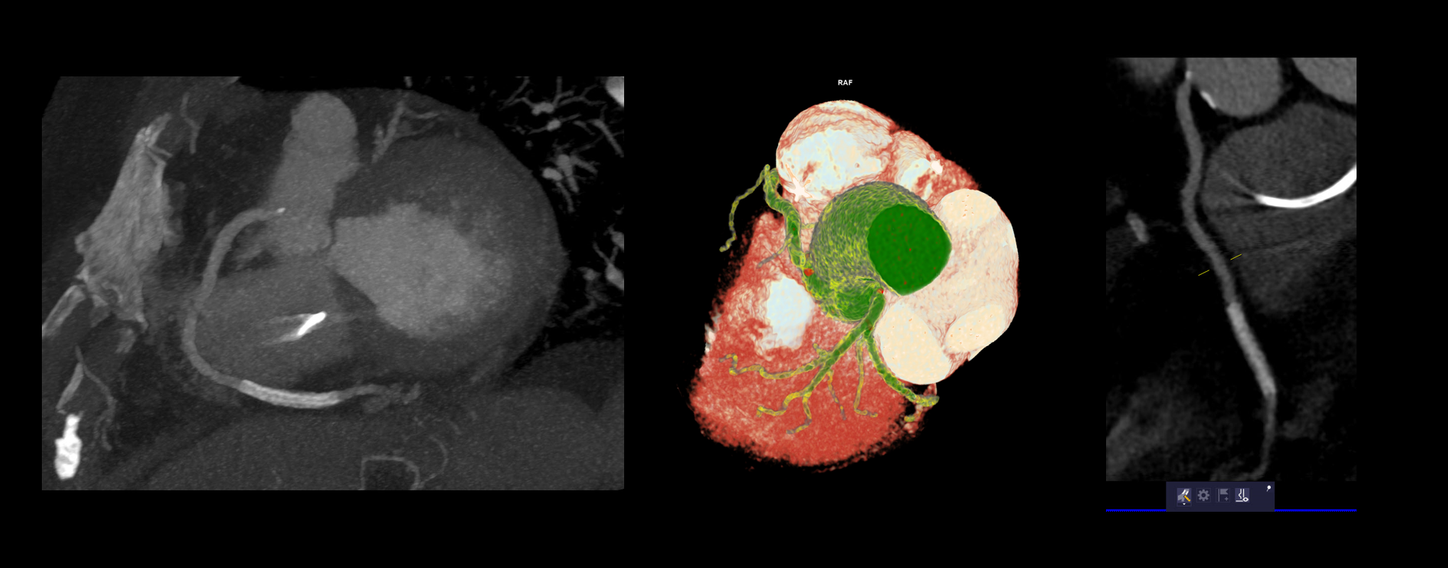
84-year-old female patient with a permanent cardiac pacemaker. Heart rate variation range during scan:102 bpm,113 bpm, 88 bpm, 80 bpm,110 bpm,132 bpm and 120 bpm. Image quality score: 5 out of 5 points.
The coronary CT angiogram was performed with the SOMATOM Force 70 kV auto mA CARE Dose4D protocol and post processed using syngo.via.
Coronary Artery Disease Assessment Conclusion: CAD-RADS 4-A/S
Non-Stented Coronary Artery Stenosis: Severe
Stenosis Stent: Minimal
In-stent restenosis Coronary Artery Stenosis Distal to Stent: None
kV - 70, ref mAs 400 , Total DLP: 388mGy*cm
Study discussion – Clinical proof 2


Case presentation
78-year-old male patient. Heart rate variation range during scan: 57 bpm, 92 bpm, 49 bpm, 56 bpm, and 95 bpm Image quality score: 5 out of 5 points
The coronary CT angiogram was performed with the SOMATOM Force 70 kV auto mA CARE Dose4D protocol and post processed using syngo.via.
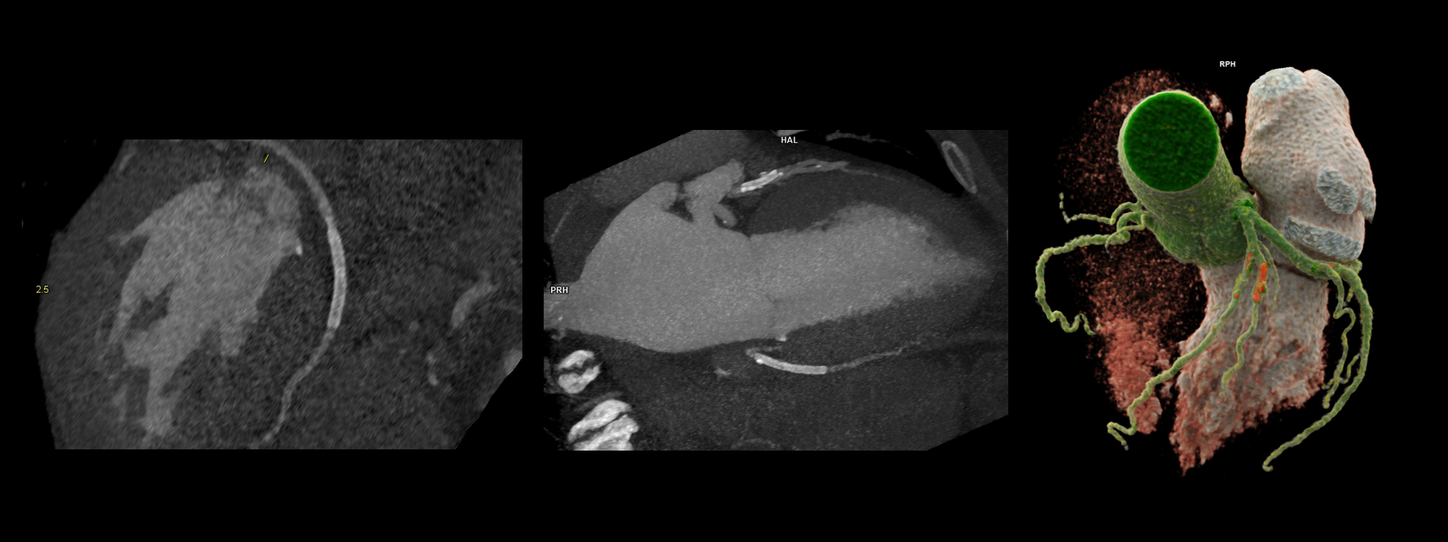
Coronary Artery Disease Assessment Conclusion: CAD-RADS 4A/S
Non-stented Coronary Artery Stenosis: Up to severe
Stenosis of LAD artery Stents: Patent 2nd diagonal artery stent and Patent PDA stent
kV - 70, ref mAs 400 , Total DLP: 388mGy*cm
Study discussion – Clinical proof 3

Case presentation
74-year-old male patient. Heart rate variation range during scan: 76 bpm to 80 bpm Image quality score: 5 out of 5 points

The coronary CT angiogram was performed with the SOMATOM Force 70 kV auto mA CARE Dose4D protocol and post processed using syngo.via.
Coronary Artery Disease Assessment Conclusion: CAD-RADS 0
Coronary Stenosis: None
Interpretation: Absent CAD
kV - 70, ref mAs 400 , Total DLP: 388mGy*cm
Discussion
Husmann et al5 performed a detailed analysis of the motion of each of the main coronary arteries throughout the cardiac cycle and determined how it varied with patient’s heart rate. At a heart rate of 60 bpm, the velocity of the right coronary artery varied from 10 mm per second to 65 mm per second over the cardiac cycle.
A high native temporal resolution in conjunction with ECG-synchronization to reconstruct the images in an optimal phase of the cardiac cycle is essential for the sharp depiction of the coronary arteries with minimum blurring from cardiac motion. This requirement is particularly of paramount importance in patients with high and variable heart rates.
A good intrinsic temporal resolution, together with selection of the optimal cardiac phase, is currently regarded as the most robust method for eliminating coronary artery motion artefacts in arrhythmic patients.
Contact

Associate Professor of Radiology,
Shahid Beheshti University of Medical Sciences, Ferdowsi Hospital, Tehran, Iran
Contact
M.Sc. of Medical Imaging,
Senior CT Clinical Specialist Ferdowsi Hospital, Tehran, Iran