
Introduction
Scanning Technique
Case Study 1
Pediatric Congenital Anomaly Imaging
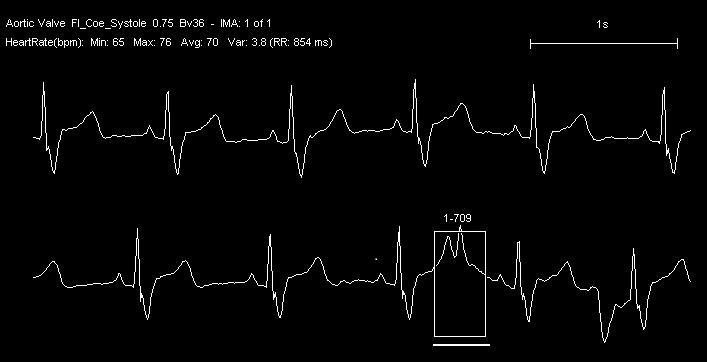
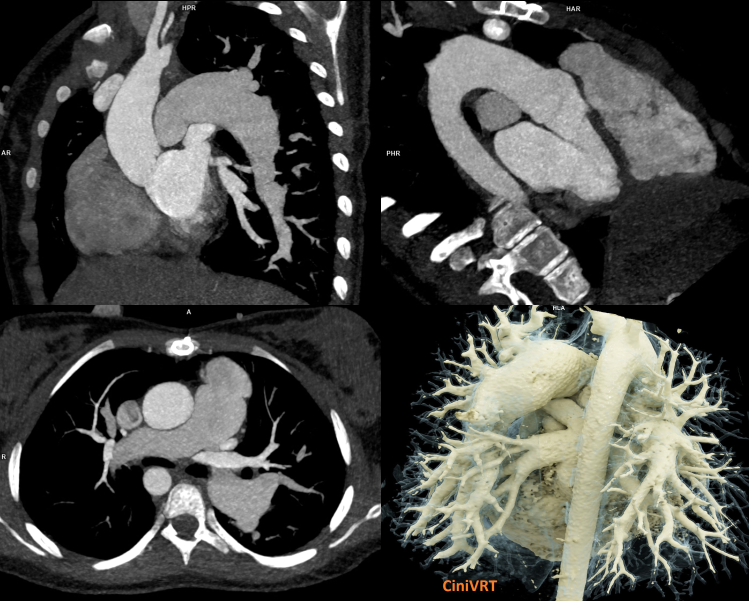
Turbo Flash mode with high-pitch enables a free-breathing, sub-second acquisition protocol. The scan length is 252.1 mm, covered in 0.41 sec scan time. The total DLP is 55 mGy*cm. Siemens CARE child solution allows performing the acquisition at 70 kV and 300
mAs, reducing the total effective dose to 0.9 mSv (with a conversion factor of 0.018).
Impression
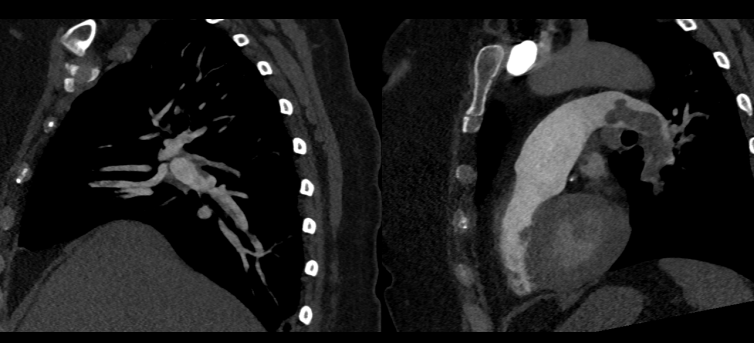
Evidence of residual infundibular pulmonary stenosis is observed. In addition, images demonstrate dilated central pulmonary arteries predominantly to the left side and dilated ascending aorta with a right-sided aortic arch.
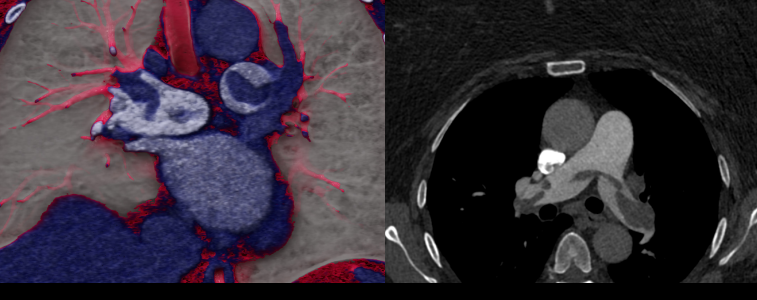
Case Study 2
Single-Beat Atrial Fibrillation imaging

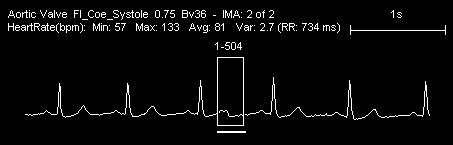
40 ml of contrast media is injected at a rate of 5.5 ml/sec. A Turbo Flash, high-pitch, single beat sub-second acquisition is performed at a CT dose index of 1.62 mGy and a total DLP of 89 mGy*cm. The scan length is 150.9 mm, covered in 0.3 sec scan time. Siemens CARE Dose 4D and CARD kV solutions allow performing the study with low contrast medium volume at 70 kV and 405 mAs, reducing the total effective dose to 1.24 mSv (with a
conversion factor of 0.014).
History
A patient suffering from hypertension presents to the emergency department with atypical chest pain and atrial fibrillation (irregular heart rate ranging from 55 to 103 BPM).
Case Study 3
Free-Breathing Pulmonary Emboli Imaging
30 ml of contrast media is injected at a rate of 5.5 ml/sec. A Turbo Flash, high-pitch, sub-second acquisition is performed at a CT dose index of 1.62 mGy and a total DLP of 89 mGy*cm. The scan length is 150.9 mm, covered in 0.3 sec scan time. Siemens CARE Dose 4D and CARD kV solutions allow performing the study with low contrast medium volume at 70 kV and 405 mAs, reducing the total effective dose to 1.24 mSv (with a conversion factor
of 0.014).
History
A patient suffering from high blood pressure, diabetes mellitus, and with BMI of 33 presents with acute shortness of breath, tachycardia, and right lower limb edema.
Conclusion
Contact

Head of the Radiology Department in NHI
National Heart Institute, Giza, Egypt

Consultant of Radiology
National Heart Institute, Giza, Egypt

Assistant fellow of Radiology
National Heart Institute, Giza, Egypt

Radiology Specialist
National Heart Institute, Giza, Egypt