Clinical Information
A 61 year old male with prior history of unstable angina, submaximal treadmill test, negative SPECT MPI, 70-80% focal disease in CX and non-flow limiting disease in LAD and RCA, calcium score of 490, diabetic, hypertensive.
Technique
Dynamic Rest myocardial perfusion PET/CT imaging was performed by injection of 15.2 mCi of NH13 Ammonia. Dynamic Stress myocardial perfusion PET/CT imaging was performed 85 minutes later, with IV administration of 0.4 mg Regadenoson followed 55 seconds later by IV administration of 15.6 mCi NH13 Ammonia. Peak heart rate response following Regadenoson injection was normal (22%); a favorable strong prognosticator. No symptomatic, hemodynamic or ECG evidence of ischemia were noted during the stress procedure.
Findings
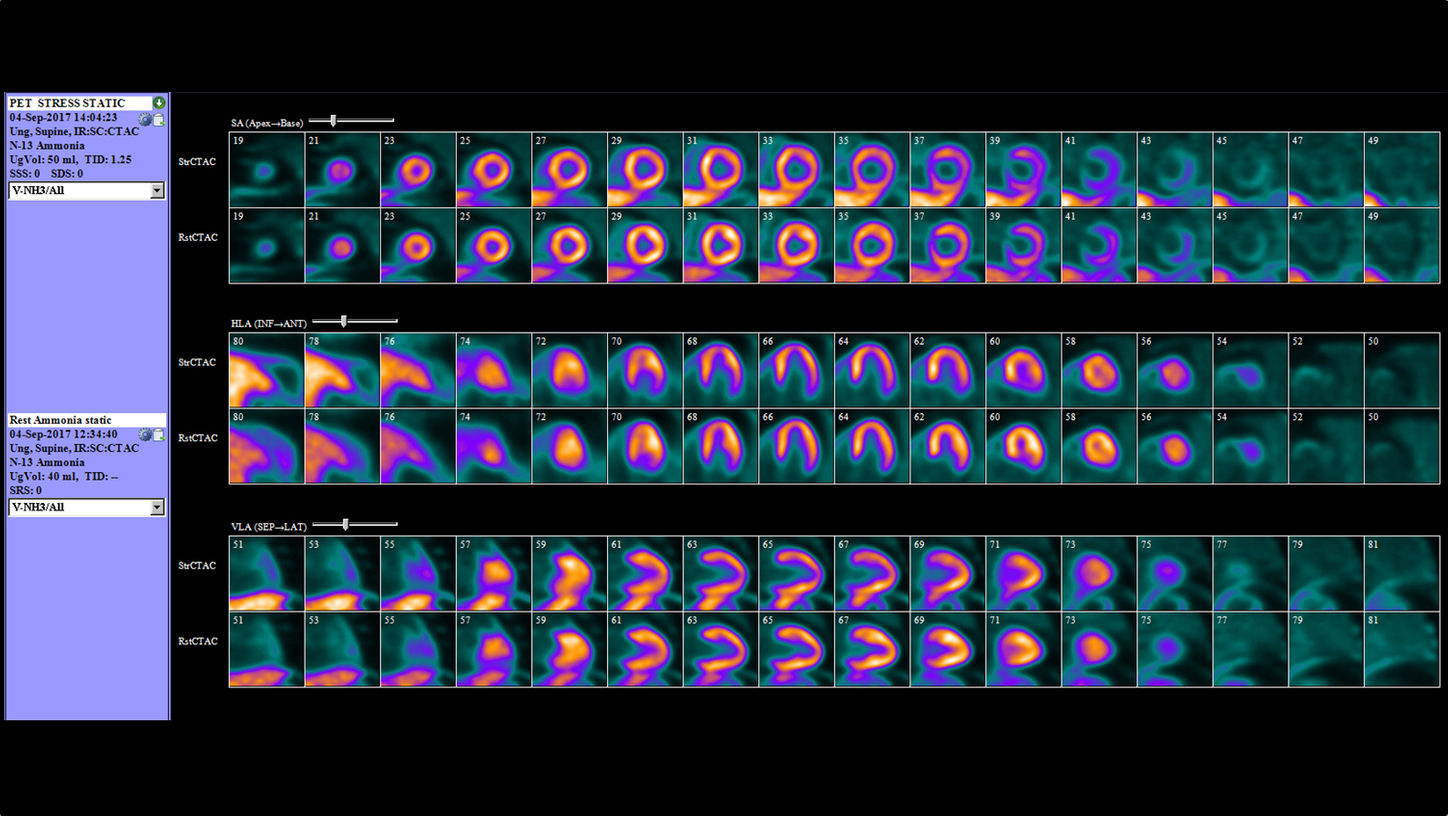
Rest and Stress PET/CT images demonstrate homogeneous tracer distribution throughout the myocardium.
Transient Ischemic Dilatation is noted (TID:1.25). Left ventricular volumes are normal on rest and stress studies. Gated PET images demonstrate normal wall motion. Estimated left ventricular ejection fraction was 72% in Peak-Stress and 75% in Rest; not demonstrating expected increase of LVEF at peak stress; consistent with impaired LVEF reserve. Note that Stress PET data represent LV function at “peak stress”.
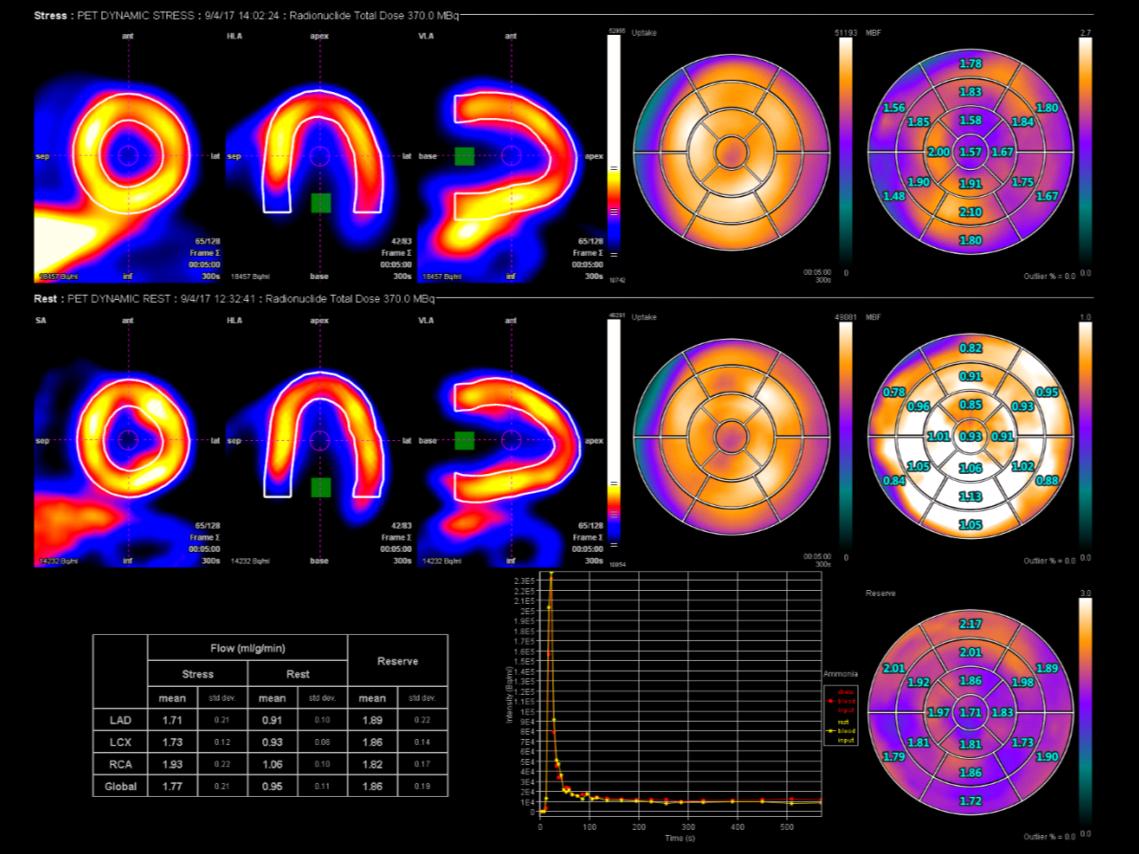
Flow reserve globally and in individual 3 territories as calculated as below: (Average Rate Pressure product at Rest : 10,090).
Contact

Impression
1. Normal “Relative” perfusion study.
2. Absolute Flow Quantification: All 3 territories demonstrate flows above ischemic thresholds of flow limiting severity (Flow limiting severity thresholds: CFR 1.7 or less, Absolute stress flow 0.91 ml/min/g or
less).
3. CFR being above ischemic threshold in CX territory rules out hemodynamically significant flow limiting lesion, previously identified as 70-80% in CTA.
4. Markedly decreased Flow Reserve (CFR below 2.0) globally and in all 3 territories; compatible with severe diffuse disease burden.
5. Evidence of non-perfusion variables associated with extensive disease burden and increased risk of hard events:
- Impaired LVEF reserve; 72% in Peak-Stress and 75% in Rest; not demonstrating expected increase of LVEF at peak stress.
- Transient Ischemic Dilatation (1.25)
Comments
This case illustrates added value of Absolute Myocardial Blood Flow Quantification over Relative MPI (Myocardial Perfusion Imaging) with either PET or SPECT. PET Absolute Flow Quantification during Rest and Peak-Stress with Coronary Flow Reserve (CFR) Calculation has incremental diagnostic and prognostic value over the traditional Relative imaging performed either by PET or SPECT.
Uniqueness of Quantitative PET MPI technique is :
1. Overcomes the shortcomings of Relative imaging with PET or SPECT. Relative imaging assumes the region with highest perfusion is normal when indeed this normal appearing region might also have visually non-apparent perfusion abnormality. Consequently, Relative imaging may lead to underestimation of the true extent of disease.
2. May define hemodynamic significance of an apparently obstructive stenosis in Angiography as illustrated in this case.
3. Superior sensitivity for Multivessel disease; 90% with PET MPI with Flow Quantification vs 71% with PET MPI alone vs 48% with SPECT MPI.
4. Looks into entire coronary tree; Focal, Diffuse and Microvascular disease and provides one composite flow measurement reflecting all of these contributors.
5. Offers more accurate diagnosis than SPECT due to:
- Higher sensitivity by utilizing tracers with higher myocardial extraction, by higher system resolution and by Peak-Stress imaging.
- Higher specificity by overcoming attenuation artifacts with higher energy photons and robust CT attenuation correction.
The outcomes by Siemens Healthineers customers described herein are based in results that were achieved in the customer’s unique setting. Since there is no ”typical” hospital and many variables exist (e.g. Hospital size, case mix, level of IT adoption), there can be no guarantee that other customers will achieve the same results.