History
A 12-year-old boy presented with pain and swelling in the right hip over a two-week duration. No fever was reported. Hip mobility was restricted and painful upon physical examination. A pelvic MRI was initially performed but was deemed inconclusive. The patient subsequently underwent a 99mTc-methyl diphosphonate (MDP) bone SPECT/CT scan using xSPECT Bone™.
The SPECT/CT study was conducted on a Symbia Intevo™ 2 system 3 hours following an intravenous injection of 16 mCi (613 MBq) of 99mTc-MDP. The initial diagnostic CT (130 kV, 26 eff mAs, 2 x 2.5 mm collimation) was followed by a SPECT acquisition (60 stops per detector, 20 seconds per stop). xSPECT Bone reconstruction was performed using CT-based zone maps. Reconstructed xSPECT Bone data was subsequently fused with CT for final interpretation.

Findings
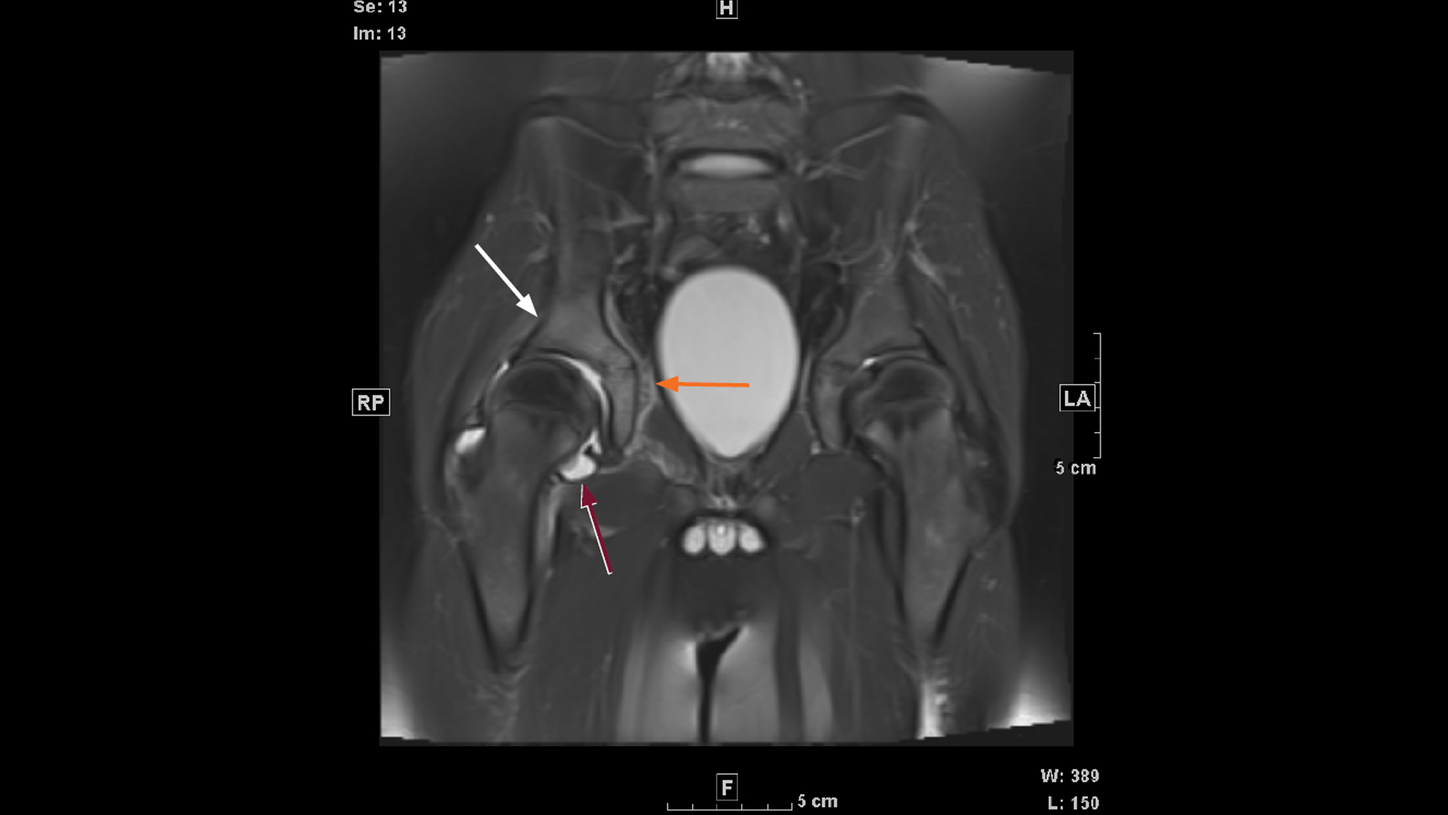
The initial MRI was performed to evaluate joint and adjacent soft tissue and acetabular marrow pathology. Figure 1 demonstrates effusion in the right hip joint with subtle marrow signal abnormality of the right acetabulum, which most likely reflects marrow edema and is suggestive of early changes of osteomyelitis. MRI images also suggest the possibility of subperiosteal abscess in the medial aspect of the acetabulum adjacent to the lateral pelvic wall. The effusion in the right hip joint seen on the MRI scan was deemed to be secondary to acetabular pathology, but septic arthropathy could not be ruled out. The absence of marrow hyperintensity on the femoral head ruled out avascular necrosis. In view of the need to distinguish between acetabular pathology and septic arthritis of the hip involving both acetabulum and femoral joint space, a 99mTc-MDP bone SPECT/CT was performed.


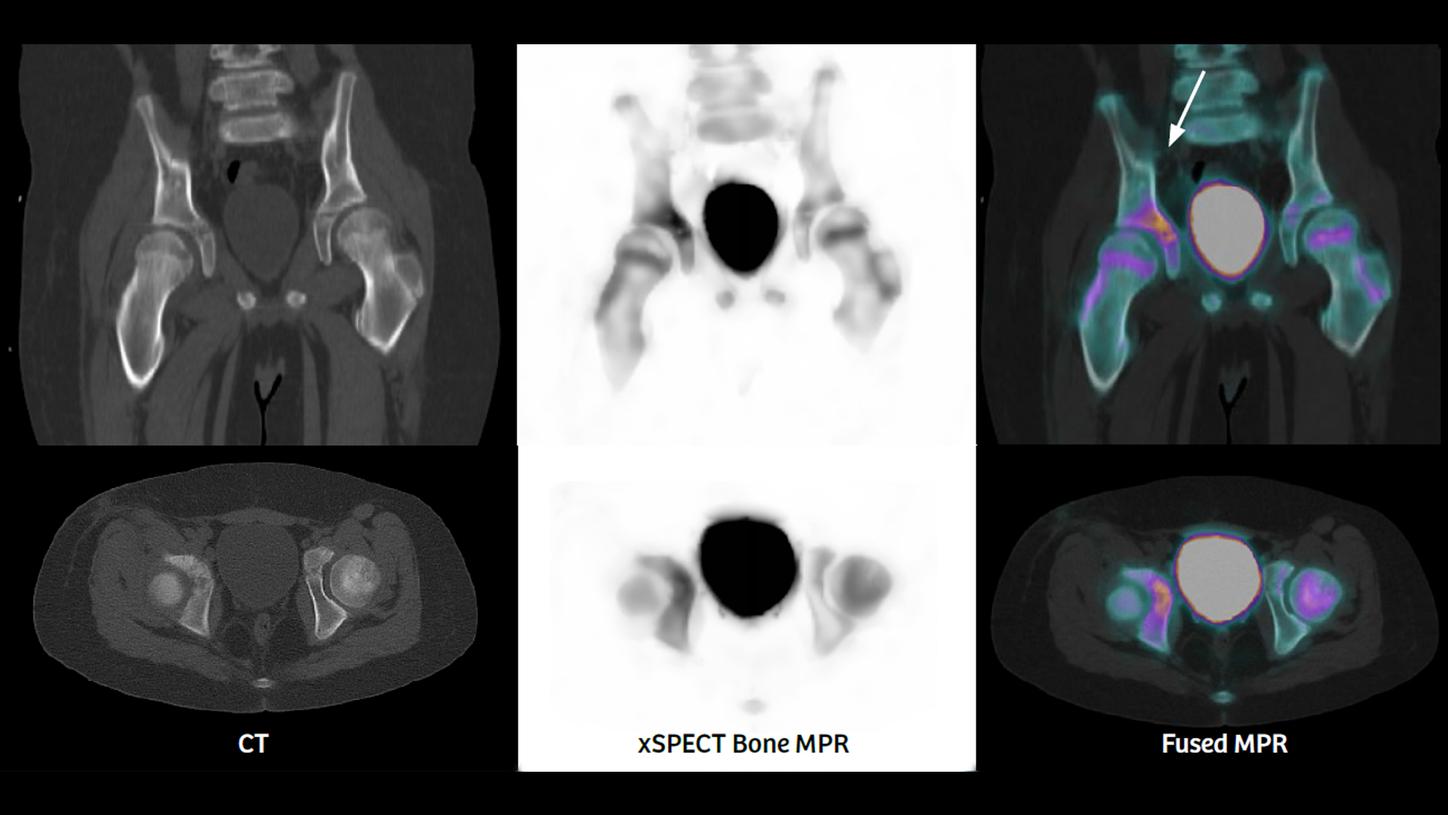
As evident from CT, xSPECT Bone, and fused images in Figures 2, 3, and 4, there is intense hypermetabolism in the acetabulum (especially the upper part just above the tri-radiate cartilage, which is accompanied by mild bony erosion with surrounding sclerosis on CT). The acetabular ossification center appears slightly hypermetabolic with fragmentation of cartilage on CT. Although the right hip joint space is only mildly enlarged, the head of the right femur does not show significant hypermetabolism. This suggests the pathology is more related to acetabulum rather than the joint space or femoral head. Such pattern of hypermetabolism and CT sclerosis is consistent with the diagnosis of early acetabular osteomyelitis.
Surgical drainage of right hip joint and obturator fossa yielded fluid which confirmed acetabular osteomyelitis in bacteriological and pathological examination. Patient was subsequently put on antibiotic therapy and physiotherapy.

Comments
Pelvic osteomyelitis is a rare form of hematogenous osteomyelitis in children.1 An uncommon entity, acetabular osteomyelitis comprises only 7-12% of all pelvic osteomyelitis cases.1,2 It is often confused with acute appendicitis.3 Early diagnosis is important for timely antibiotic therapy, with or without surgical intervention, in order to avoid permanent hip joint defects, avascular necrosis of femoral head, and acetabular deformities.
In this patient, hypermetabolism in the upper acetabulum adjacent to and above the tri-radiate cartilage (as shown by intense 99mTc-MDP uptake) was key to suspicion of acetabular osteomyelitis in the absence of corresponding hypermetabolism in the head of right femur.
CT delineation of mild erosion of the upper acetabulum corresponding to the highest intensity of hypermetabolism as delineated on xSPECT Bone with adjacent sclerosis was also supportive evidence pointing towards acetabular pathology.


Conclusion
In a 12-year-old boy with pain and restriction of mobility in the right hip joint, sharp definition of acetabular hypermetabolism by xSPECT Bone—in correlation with findings of CT and MRI—helped arrive at the diagnosis of acetabular osteomyelitis.