Abstract
Technical difficulties to find true lumen of the occluded vessel exists in CTO PCI cases. Lately, technology has enabled doctors to use the images of CT coronary angiogram in the cath lab to guide complex coronary intervention. Simultaneously, efforts to limit the volume of contrast media usage and Xray exposure time across the Cat Lab continues.
The following cases shall demonstrate how CTO guidance plays an important tool in enhancing the evaluation, planning, and treatment of a CTO vessel. Also, with CT coronary angiogram and coronary angiogram images fusion in a less complex case led to minimizing potential complication, less contrast media usage, and reduced Xray exposure time.
Case One
A 55-year-old, heavy smoker with mildly elevated cholesterol (total cholesterol 221, LDL 194) and positive family history presented to cardiac centre complaining of chest pain on exertion. His exercise tolerance is reduced to less than 500 meters on exertion. No history of diabetes or hypertension.
Coronary angiogram later showed severe subtotal occlusion in a moderate size ramus branch and total long chronic total occlusion in the RCA extending from proximal segment to the distal segment of the vessel at the level of PDA/PLV bifurcation. LM, LAD and circumflex arteries were normal.

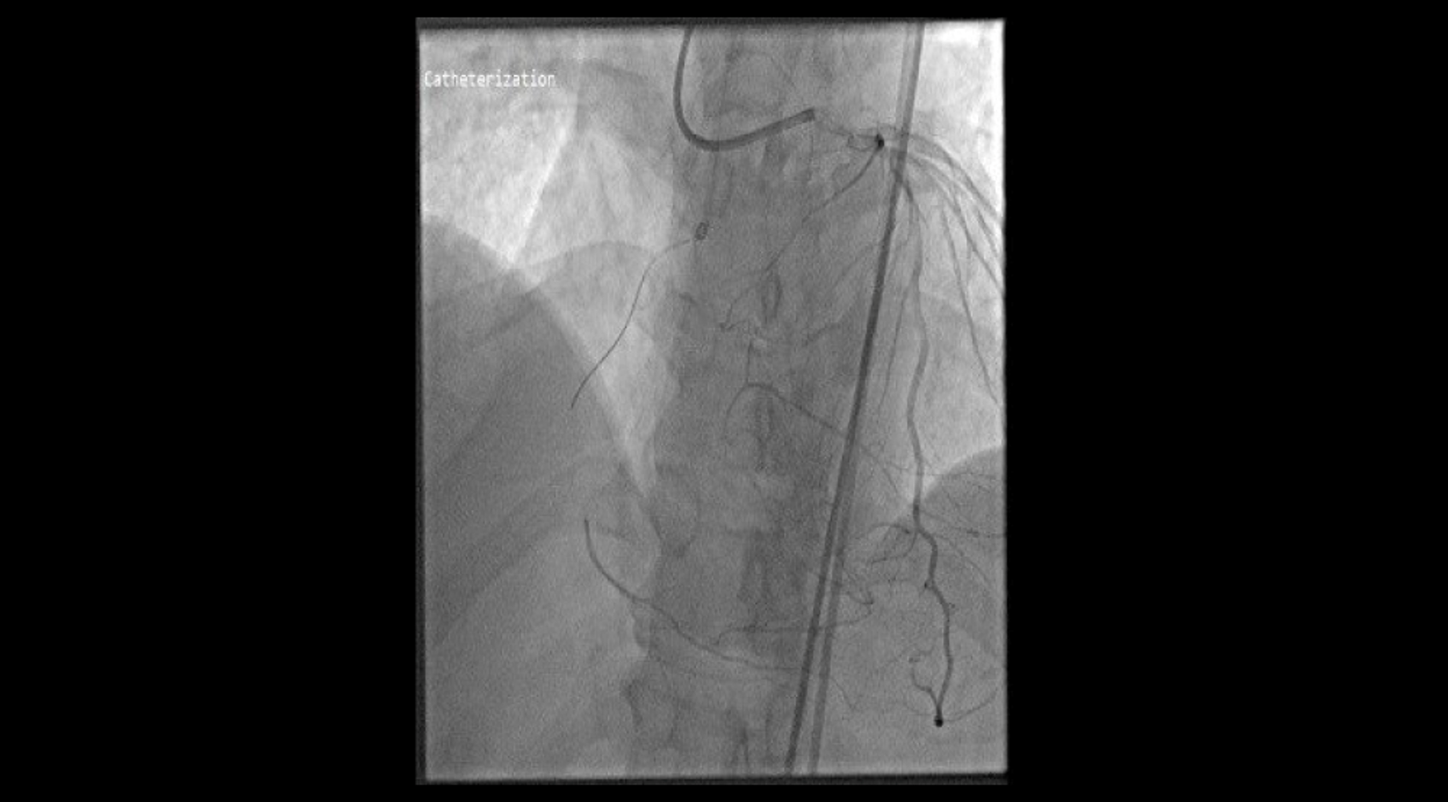
Coronary Angiography of RCA pre-PCI
Treatment
PCI to ramus branch was through right radial access (RRA). The decision was to attempt RCA CTO, a second 6F femoral access to attempt RCA anterogradely and the RRA access to assess the distal vessel.
Procedure was long and complicated with RCA multiple dissections and sub intimal tracking. The procedure was abandoned at that stage due to the high usage of contrast. Patient was assessed in the clinic 3 weeks post procedure and he reported improvement but not complete resolution of symptoms. Patient was still complaining of chest with limited exercise tolerance. Clinical decision was to redo PCI to RCA.
Before performing the PCI, further assessment with CT coronary angiogram for better planning of the CTO procedure was done utilizing syngo CTO Guidance clinical software application.
Wire attempts to engage CTO track.

PCI was attempted using right femoral artery for anterograde and left femoral artery for retrograde/ collaterals assessment with live 3d road map from CT coronary angiogram fused images to assess the occluded track of the RCA during PCI.

Distal wire position confirmation.


Final PCI results with patent right coronary artery (RCA).
Procedure was successful in a relatively short time (total procedure time 60 minutes, screening time 36 minutes) and low contrast media usage (130 milliliter). No complications reported post procedure.
Case Two
A 50-year old man presented with atypical chest pain. Risk factors for coronary artery disease include smoking 1 pack a day for 35 years and mild hypertension. He reported reduced exercise tolerance in the last two months due to breathlessness.
Physical examination reported as normal with exception of blood pressure readings 145/85.ECG and echocardiogram were normal. As he was atypically symptomatic, CT coronary angiogram was done, which reported mildly calcified vessels (calcium score 58); normal LM, circumflex and right coronary artery. LAD showed significant lesion in the middle segment involving a middle size diagonal branch.
Patient was symptomatic with secondary prevention and anti-angina medications. Coronary angiogram was performed which confirmed the findings.

PA cranial image from cath lab.

Planning for PCI:
As CT angiogram images were available, the images were merged into Siemens Healthineers Artis Q syngo CTO Guidance software which automatically adds centerlines to the segmented coronary arteries from CT angiogram with color coding showing how orthogonal C-arm to the vessel segments and enabled us to overlay these segmented arteries on live fluoroscopy using 3D dynamic Roadmap throughout the procedure for guidance. This led to detect lesion anatomical landmarks with reduced contrast usage and less radiation. The approximate vessel size, length of the lesion and side branch assessment was done through the software.


Conclusion on using Siemens Healthineers syngo CTO Guidance software across the cath lab:
• It helps to understand the morphology of the lesion, the length of the lesion, calcifications, and tortuosity.
• Facilitates the best projection for lesions.
• Selects the right projection for better visualization of the target lesion without radiation.
• Radiation exposure is suspected to be reduced by 30-40%.
• Potentially less complications with higher success rate.
• Reduction in the X-Ray dose during the procedure.

Final PA cranial image from cath lab.


Contact

Consultant Interventional Cardiologist
Arab Medical Center, Amman, Jordan
Contact

Manager Cath Lab Department,
Arab Medical Center, Amman, Jordan